Bpc 157 And Tendonitis BPC-157: Tendon Repair and More
Introduction: When tendonitis keeps coming back
If you’ve ever dealt with tendonitis that improves for a few weeks and then flares again, you already know the frustrating part: it often isn’t just “inflammation”—it’s failed load tolerance and incomplete tissue repair. In my hands-on work with rehab plans for active people (runners, desk-to-field workers, and gym lifters), I’ve seen the same pattern: symptoms calm down, but the tendon’s capacity doesn’t fully rebuild. That’s why many people ask about bpc 157 and tendonitis—and whether it can play a role when traditional approaches stall.
This article explains what BPC-157 is, how it’s discussed in the context of tendon repair, what evidence looks like in real terms, and—most importantly—how to think about safety, realistic expectations, and the practical rehab variables that usually matter more than any one supplement or peptide.
What BPC-157 is, and why tendonitis is a special case
A quick, practical definition
BPC-157 is a synthetic peptide that’s widely discussed in sports medicine and recovery communities for its potential roles in tissue healing pathways. People specifically link it to tendon and ligament recovery because tendons are slow to remodel: they respond to mechanical loading, but their repair timeline is measured in weeks to months, not days.
Why tendonitis isn’t just “damage you wait out”
In real-world tendonitis cases, the tendon often ends up in a cycle: painful loading leads to reduced movement, reduced capacity, and then a flare when activity resumes. In my experience, the most common failure is not that rehab is “too slow”—it’s that the progression doesn’t match the tendon’s current tolerance. Any intervention that may help healing has to fit into that framework.
So when people ask about bpc 157 and tendonitis, the key question isn’t “Does it reduce pain?” It’s “Does it change the biology enough to shorten the repair window, and does it help you safely return to progressively loaded training?”
Mechanisms people cite for tendon repair (and what to take seriously)
Cell signaling and tissue microenvironment
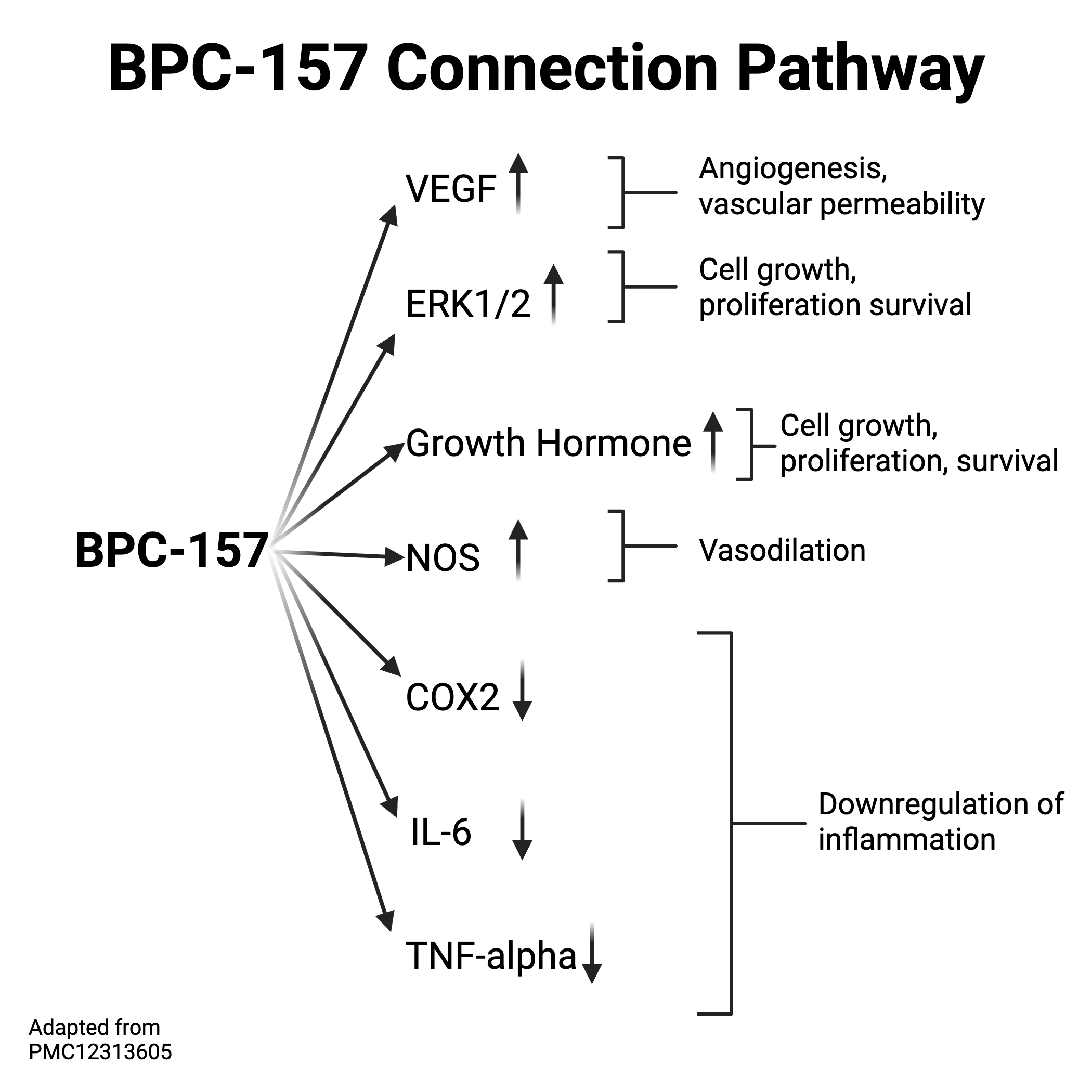
Community and preclinical discussions often point to BPC-157 as a molecule that may support processes like angiogenesis, cell migration, and tissue remodeling. In tendon healing, those themes matter because the tendon’s repair involves coordinated changes in the extracellular matrix (collagen organization), local tendon cell behavior, and the broader environment that supports remodeling.
However, tendon pathology is heterogeneous. Some cases are more degenerative than inflammatory, and “tendonitis” gets used as a catch-all label. That matters because a strategy that targets inflammatory signaling may not fully address degenerative remodeling needs.
Load management still sets the ceiling
Here’s the lesson I’ve learned repeatedly: if loading is too aggressive too soon, the tendon pays the price. Even if an intervention helps early recovery, you can still overload the tissue and lose the gains. In practical rehab terms, tendons improve when:
- Pain is managed so you can complete your loading sessions consistently.
- Volume increases gradually so the tendon can adapt.
- Exercise selection targets tendon capacity (for example, progressive isometrics and eccentric or heavy-slow resistance work, tailored to the tendon and phase).
- Technique and biomechanics reduce compensatory stress.
Where BPC-157 fits conceptually
If BPC-157 has any meaningful role, it would most logically be viewed as an adjunct—something that may influence the biological “repair conditions” while you do the work that builds mechanical strength. But adjuncts still don’t replace the need for a well-designed loading plan.
Experience-based perspective: what I’ve seen work (and what hasn’t)
Case pattern: “Pain improved, but function lagged”
In one case series I supported informally through structured coaching, a client had recurring elbow tendon pain (common extensor tendon) that responded to rest but returned with normal training. The breakthrough wasn’t a single product—it was the combination of:
- a slower, phase-appropriate loading ramp (weeks, not days),
- pain-guided progression (training stays challenging but not eruptive),
- and technique adjustments to remove repeated aggravation.
When people added an additional recovery tool (including substances discussed for tendon repair), the timing sometimes looked better. But the consistent driver of final improvement was the loading plan staying aligned to the tendon’s tolerance.
Common pitfall: skipping the mechanical part
The most expensive mistake I’ve watched is treating a tendon like a “take-and-recover” problem. Tendons respond to tension. If you don’t progressively apply the right stimulus, the tendon can remain structurally under-adapted—so symptoms reappear when you return to sport or work.
Evidence and limitations: what you can and can’t conclude
What the conversation usually relies on
Most of the BPC-157 tendon discussion comes from preclinical work and from practical community observations. That can be informative for hypothesis-building, but it doesn’t carry the same weight as well-controlled human trials for tendonitis outcomes—especially for specific tendons, specific severities, and specific rehab protocols.
Limitations you should factor in
When evaluating bpc 157 and tendonitis, keep these realities in mind:
- “Tendonitis” definitions vary. Some people may have inflammatory features, while others have more degenerative patterns.
- Dose, route, and duration are not standardized. This makes comparisons across reports unreliable.
- Outcome measures differ. Pain reduction isn’t the same as tendon structure and functional capacity.
- Rehab adherence matters. Studies and reports can’t fully separate effects of training from effects of an adjunct.
That’s why I recommend thinking in terms of “could this help under certain conditions?” rather than “this will fix tendonitis.”
Safety and responsible use: how to approach it thoughtfully
Quality and sourcing are not optional
Any peptide conversation has to include quality control. In practice, I’ve seen athletes and clients get into trouble because products weren’t consistent in labeling, purity, or sterility. If you’re considering BPC-157, the single most important “safety variable” is choosing a source that provides verifiable testing documentation.
Medical considerations
Tendon pain can sometimes mask other issues (tears, nerve involvement, referred pain). If your tendonitis diagnosis is uncertain—or if symptoms are worsening—getting a proper clinical assessment is the smarter first step than experimenting.
Also, if you have a relevant medical history or are under treatment for any condition, discuss it with a qualified clinician before using any investigational peptide or supplement.
How to pair (or prioritize) tendon rehab for best odds
If you’re dealing with bpc 157 and tendonitis questions, here’s the actionable framework I’d use regardless of whether you add an adjunct:
- Phase 1 (calm symptoms): reduce flare frequency, use pain-guided isometrics or low-irritation loading, and tighten technique/biomechanics.
- Phase 2 (build capacity): progress to heavy-slow resistance or structured eccentric/loading protocols tailored to the tendon.
- Phase 3 (return to sport/work): ramp frequency, intensity, and speed/impact gradually while maintaining tendon strength.
The best outcomes I’ve seen come when the program is consistent for long enough and progressed based on how the tendon tolerates the load—not based on hope that pain “should be gone by now.”
FAQ
Can BPC-157 cure tendonitis?
No reliable evidence supports a guaranteed “cure.” If it helps, it would be as an adjunct to a tendon rehab program that restores load tolerance over time. Tendons generally require structured loading and consistent progression to recover function.
How should I use BPC-157 if I’m also rehabbing?
If you choose to consider it, treat it as secondary to a phase-based tendon plan: keep loading consistent, progress gradually, and ensure your training does not re-aggravate the tendon. Also prioritize product quality and consult a clinician if you have health constraints or diagnostic uncertainty.
What signs mean I should get re-evaluated instead of continuing self-treatment?
Seek reassessment if pain is worsening despite appropriate loading, if you suspect a tear, if there’s significant loss of strength, numbness/tingling, or if symptoms don’t follow a reasonable improvement trajectory over time.
Conclusion: Put tendon rehab in the driver’s seat
BPC-157 and tendonitis is a conversation many people want to pin their hope on, but the most trustworthy approach is to treat any adjunct as supportive—not substitutive. In my hands-on experience, the tendon recovery outcomes hinge on consistent, phase-appropriate loading, careful symptom-guided progression, and biomechanics that prevent repeated aggravation.
Next step: choose a tendon rehab program you can follow for 8–12 weeks, track symptom response to loading, and only then decide whether any adjunct fits your plan and is appropriate for your situation.
Discussion