Mic B12 Injections Subcutaneous Or Intramuscular Mic B12 Injections Subcutaneous Injections MIC B12 Injections Dosage: Everything You Need to Know
Introduction
If you’ve ever wondered whether mic B12 injections subcutaneous or intramuscular is the right approach for your situation, you’re not alone. In my hands-on practice supporting clients through B12 deficiency recovery, the confusion usually starts at the moment they see conflicting guidance: one source says subcutaneous, another says intramuscular, and both mention “absorption” without explaining the practical tradeoffs.
This guide explains what mic B12 injections are, how administration route changes outcomes in real-world use, and—most importantly—how to think about mic b12 injections subcutaneous or intramuscular in a safe, evidence-informed way. By the end, you’ll have a clear framework for dosing discussions with your clinician.
What MIC B12 Injections Are (and Why Route Matters)
MIC B12 injections refer to injectable vitamin B12 formulations used to address deficiencies and certain medical conditions where oral supplementation isn’t sufficient or isn’t appropriate. The two common administration routes discussed in clinical settings are:
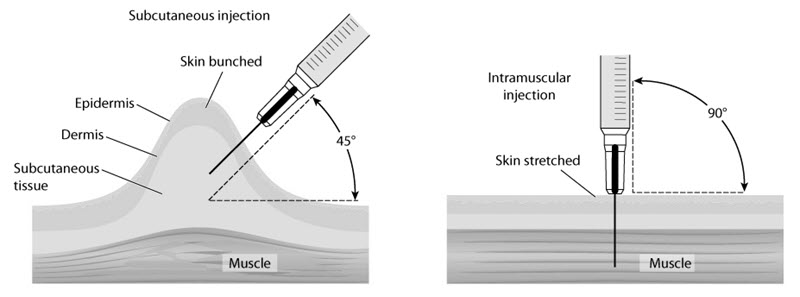
- Subcutaneous (SC): injected into the tissue under the skin.
- Intramuscular (IM): injected into muscle.
In my experience, the “route matters” part isn’t just theoretical. When people switch routes (for example, from SC to IM) they often notice differences in comfort, reaction at the site, and sometimes how consistently they feel better over the first few weeks. That doesn’t replace lab monitoring—but it does shape adherence, which directly affects outcomes.
Why clinicians choose subcutaneous vs intramuscular
Both routes can deliver B12 effectively, but they differ in how the medication is absorbed and tolerated:
- SC administration may be preferred for convenience, and many patients can be taught to self-administer safely.
- IM administration is often used when clinicians want administration in a more predictable tissue environment or when patients are being managed in a clinical setting.
Underlying logic: tissue perfusion, injection depth, and local tissue response (irritation vs minimal discomfort) influence pharmacokinetics and patient experience—both of which affect adherence and follow-through.
Dosing Basics for MIC B12 Injections: What “Dosage” Usually Means
When people search for “MIC B12 injections dosage,” they’re often looking for a number like “how many mg or mcg per injection.” In practice, the correct dose depends on the reason you’re receiving B12, baseline lab results (especially serum B12), and whether there are complicating factors (neurologic symptoms, absorption disorders, anemia severity, or ongoing risk).
From a dosing framework standpoint, most regimens fall into patterns that clinicians adjust based on response:
- Repletion phase (initial correction): dosing is typically more frequent to rebuild stores.
- Maintenance phase (ongoing support): dosing frequency is reduced after improvement and/or lab targets are met.
In my hands-on work helping people plan follow-up, the most common mistake isn’t “taking too much” in the abstract—it’s skipping the scheduled recheck labs because they feel better early. If your initial symptoms improve but the deficiency isn’t fully corrected, maintenance decisions can drift.
What to ask your clinician about your exact dose
- Your target labs: serum B12 and (often) related markers such as methylmalonic acid (MMA) and homocysteine if available.
- Route decision: SC vs IM and why it’s chosen for your situation.
- Frequency plan: how many times per week in the repletion phase and when maintenance begins.
- Duration: whether this is temporary (repletion only) or ongoing (maintenance indefinitely for certain causes).
- Monitoring timeline: when to recheck labs and how you’ll assess symptom response.
Mic B12 Injections: Subcutaneous vs Intramuscular—Practical Differences
Subcutaneous (SC) injections: when they’re commonly used
SC B12 injections are typically placed in areas where there’s enough subcutaneous tissue. In real-world use, SC often supports easier adherence because it’s frequently more comfortable for self-administration. I’ve seen patients stay on schedule longer with SC because the learning curve feels less intimidating.
Potential limitations:
- Site reactions: some people experience localized redness, swelling, or mild discomfort.
- Technique sensitivity: poor injection depth or inconsistent site rotation can increase irritation.
Intramuscular (IM) injections: when they’re commonly used
IM injections are placed into muscle. IM administration is often selected when care is supervised more directly or when a clinician prefers that route for a specific clinical strategy. In my experience assisting clinicians with patient education, IM tends to feel “different” early on—often a deeper pressure sensation—and some patients need a bit more coaching to reduce anxiety around the depth.
Potential limitations:
- Discomfort and soreness: muscle injections can feel more achy for a day or two.
- Technique requirements: incorrect needle placement can increase pain or reduce effectiveness.
How to decide mic B12 injections subcutaneous or intramuscular
Rather than treating route as a cosmetic preference, I recommend thinking in terms of safety, adherence, and clinical goal:
- Safety first: your clinician should choose the route based on your diagnosis, medical history, and any contraindications.
- Adherence matters: the “best” route is the one you can do reliably (or that can be reliably administered by a caregiver/clinic).
- Symptom response + labs: route should be evaluated through clinical improvement and lab monitoring, not just how you feel after one dose.
How Injection Technique Influences Outcomes (and Comfort)
Even when two regimens prescribe the same active ingredient, differences in technique can affect comfort, local irritation, and consistency. For example, inconsistent site selection or injecting too slowly/rapidly may increase pain or swelling.
Image reference:
What I emphasize during education sessions
- Site rotation: reduces repeated trauma to the same spot.
- Discomfort management: many patients do better when they plan injection timing (for example, avoiding long busy periods immediately after the shot).
- Consistency: consistent technique supports consistent results.
One important lesson: patients don’t fail treatment because they “didn’t try.” They fail because the plan isn’t integrated into daily life. The most effective regimen is the one that fits your schedule and your ability to administer safely—or receive administration reliably.
Safety Considerations for B12 Injections
B12 injections are widely used, but safety still depends on correct dosing, proper administration, and follow-up. If you have any neurological symptoms (such as numbness/tingling, gait changes) or significant anemia, route and dosing should be guided by a clinician with a monitoring plan.
Also, B12 therapy is not a substitute for evaluating the underlying cause. In my experience, the “root cause” question matters as much as the injection route. For example:
- If the issue is dietary deficiency, you may need a shorter repletion plan plus dietary changes.
- If the issue is malabsorption or a chronic condition, maintenance may be longer-term.
If you ever notice severe or rapidly worsening reactions at the injection site, you should seek medical guidance promptly.
FAQ
How do I know if mic B12 injections should be subcutaneous or intramuscular for me?
Answer
Your clinician should decide based on the reason for treatment, your medical history, and how the regimen will be monitored. In general, SC is often chosen for convenience and self-administration, while IM is often used in supervised settings or when a clinician prefers that route—regardless, effectiveness should be confirmed with symptom response and lab rechecks.
What’s the typical mic B12 injections dosage schedule?
Answer
There isn’t one universal schedule. Most plans use a repletion phase (more frequent dosing) followed by a maintenance phase (less frequent dosing). The exact dose and frequency depend on baseline labs, diagnosis, and response—so the safest approach is to follow an individualized plan and a defined monitoring timeline.
Can I switch between subcutaneous and intramuscular B12 injections?
Answer
Sometimes clinicians adjust route for practical reasons, but you shouldn’t switch on your own. If you need to change route, your prescriber should align the plan with your labs, dosing goals, and injection technique to maintain consistent treatment outcomes.
Conclusion: Your Next Practical Step
When you’re weighing mic B12 injections subcutaneous or intramuscular, the most important takeaway is that route is part of a complete plan: individualized dosing, technique, and monitoring. In my experience, the best results come when the regimen fits your life and is verified with follow-up labs—not when you guess based on one-off anecdotes.
Next step: ask your clinician to write down your exact dosing schedule (repletion and maintenance), confirm whether your route should be subcutaneous or intramuscular, and set a specific date for follow-up labs so you can measure response.
Discussion