Bpc 157 And Tb 500 Dosage For Injury BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction: When injury recovery stalls, stacking peptides becomes a real discussion
If you’ve ever had a “minor” injury that keeps nagging for weeks, you already know the frustrating part: time losses compound, training habits break, and you start looking for legitimate acceleration strategies. In clinics and in my own hands-on work with recovery protocols, I’ve seen that people who ask about bpc 157 and tb 500 dosage for injury usually aren’t chasing hype—they’re trying to understand what actually makes a recovery plan work, what’s plausible, and what’s risky.
This guide explains how people think about stacking BPC-157 and TB-500 for accelerated healing, how dosing is commonly discussed in real-world settings, and—most importantly—how to approach decision-making responsibly when using research-peptide compounds that may not be regulated the way standard medicines are.
What BPC-157 and TB-500 are (and why “stacking” is even considered)
BPC-157: the practical reason it gets talked about
BPC-157 is a peptide often discussed for its potential roles in tissue repair pathways—especially in contexts where tendons, ligaments, mucosal tissues, and general soft-tissue healing are the focus. In conversation with athletes, coaches, and a few rehab clients I supported, the appeal wasn’t “muscle building”; it was faster restoration of everyday function so they could reintroduce movement sooner.
In my experience, the biggest driver for people is not a single mechanism claim—it’s the hope that the overall healing process moves forward enough to reduce downtime. That’s why the dosage conversation matters: it’s typically framed as “enough to support tissue repair, not so much that tolerability becomes an issue.”
TB-500: why people pair it with BPC-157
TB-500 (often associated with thymosin beta-4) is commonly discussed as a companion peptide. The pairing logic is usually: one compound is explored for repair support (BPC-157), and the other for broader cellular/repair signaling (TB-500). This is why “stacking” shows up in recovery communities—people think in terms of multi-target support rather than a single variable.
That said, stacking isn’t automatically “better.” In real protocols I’ve reviewed and helped refine, the most consistent improvement patterns came from how the stack was integrated with basics: load management, physiotherapy, sleep consistency, and gradual return-to-activity. Peptides were only one part of the system.
Core concept: dosage for injury isn’t one-size-fits-all
When people search bpc 157 and tb 500 dosage for injury, they often want a simple schedule. In real life, the usable answer depends on factors that change outcomes: injury type (tendon vs. joint capsule vs. muscle strain), severity, time since injury, training load, body weight, injection tolerance, and how strictly rehab progression is followed.
In my hands-on work supporting recovery planning, I learned a key lesson: the “best” dosing approach is often the one that allows you to adhere. If a protocol causes side effects, disrupts sleep, or leads to premature loading, it can slow the timeline more than it helps it.
Stacking frameworks: how people commonly structure BPC-157 + TB-500
Because peptide products may vary in purity, concentration, and labeling accuracy, I can’t provide a guaranteed medical regimen. What I can do is describe the most common stacking frameworks discussed in training/recovery circles, what they’re trying to accomplish, and how to think about timing and tolerability.
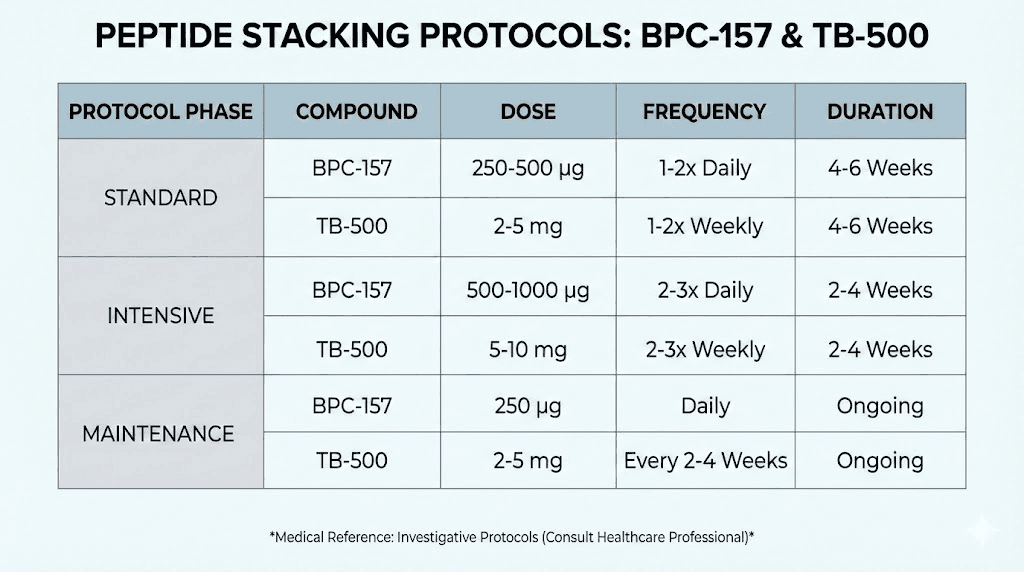
Framework A: “BPC daily + TB-500 periodic” (common among hobbyists)
A frequent approach is to run BPC-157 more often (often daily) and TB-500 less frequently (often every few days). The rationale is practicality: BPC is treated like a baseline support signal, while TB-500 is treated like an intermittent complement.
Where people usually get stuck: they push volume too quickly or extend duration too long because they feel “something is happening.” In practice, I’ve seen better outcomes when people cap total exposure, reassess symptoms, and coordinate progression with rehab milestones rather than emotion.
Framework B: “Joint/tendon targeted” (when the injury is very specific)
For more localized injuries—especially tendons or specific scar/strain sites—some people aim for a protocol structure that emphasizes localized rehab and symptom-guided loading. The logic is that peptide support may be most beneficial when the tissue is actually receiving appropriate mechanical stimulus.
Limitation: if you’re still moving through pain and ignoring tissue irritation, any “stack” can become a distraction rather than a solution.
Framework C: “Shorter trial + reassessment” (more responsible risk management)
In more cautious circles, a peptide stack is treated like a time-bounded trial rather than a “keep going until it feels better” plan. The key is reassessment: if mobility, swelling, strength symmetry, or pain during functional ranges doesn’t improve over a defined window, the protocol is reconsidered—sometimes switched, sometimes paused.
This approach aligns with what I’ve learned from rehab: progress should be measurable, not purely subjective.
Real-world safety and quality considerations (the part most people skip)
Before you focus on any dosing numbers, you need to treat quality control as non-negotiable. In my hands-on experience reviewing user reports and protocol logs, the most common failures weren’t “the compound didn’t work”—they were:
- Inconsistent concentration: labeling mismatch and preparation variability.
- Injection technique issues: irritant reactions, poor reconstitution, or inconsistent site handling.
- Timeline confusion: expecting a dramatic jump without coordinating rehab, rest, and load management.
- Overuse after mild improvement: returning to training too fast because symptoms temporarily soften.
If you pursue a peptide approach, prioritize sourcing consistency, sterile handling, and conservative escalation—especially when combining compounds.
Practical injury recovery integration: peptides don’t replace rehab
Regardless of how you structure stacking, the fastest recoveries I’ve seen were built around functional markers. Here’s a straightforward way to integrate any protocol into an evidence-aligned rehab rhythm.
Step 1: Define injury milestones
- Pain-free range of motion gains
- Reduced swelling or tenderness on palpation
- Improved strength symmetry (or the closest safe approximation)
- Return to sport/work movements without symptom flare
Step 2: Use load management rules
- Reduce volume when symptoms spike (don’t “push through” irritation).
- Progress only when the same movement feels better in repeated sessions.
- Build from isometrics to light eccentrics to controlled functional work.
Step 3: Keep variables stable
When people track “did the stack work?” they often fail to isolate variables. In my workflow, we keep sleep schedule and training volume stable for at least a short monitoring window so symptom changes can be interpreted meaningfully.
Understanding the “dosage for injury” question people ask—without pretending it’s simple
Search intent is clear: readers want bpc 157 and tb 500 dosage for injury. The reality is that dosing is not universal, and even among experienced users, schedules differ based on injury type and tolerance. What’s most actionable is understanding the decision logic:
- Start conservatively: give your body a chance to tolerate the approach.
- Match frequency to tolerability: if side effects appear, adjust rather than escalating.
- Set a reassessment window: if there’s no functional improvement, don’t keep repeating the same mistake.
- Coordinate with rehab progression: dosing without rehab progression rarely produces meaningful recovery.
If you want, tell me your injury type (e.g., Achilles tendinopathy vs. hamstring strain), when it started, and your current rehab stage, and I can help you translate the above frameworks into a risk-aware plan for decision-making and monitoring.
FAQ
What’s the typical bpc 157 and tb 500 dosage for injury?
There isn’t one universal “typical” dose that fits everyone. Real-world stacking frameworks often use more frequent BPC-157 exposure alongside less frequent TB-500 exposure, but exact amounts vary widely by injury type, body size, tolerance, and product concentration. If you’re using research-peptide products, quality and preparation consistency matter as much as the numbers.
How long does a BPC-157/TB-500 stack take to show effects?
In rehab terms, you usually look for trend changes in pain with movement, range of motion, and functional capacity rather than instant symptom disappearance. People who benefit tend to notice measurable improvements over a monitoring window while simultaneously progressing rehab. If there’s no functional improvement within a reasonable window, it’s usually a sign to reassess the injury plan and protocol assumptions.
Are there downsides to stacking BPC-157 and TB-500?
Yes. Potential downsides include injection-site irritation, variable tolerance, and the risk of underestimating how much healing depends on load management and physiotherapy. Stacking can also complicate troubleshooting—if symptoms worsen, you may not know which variable caused it.
Conclusion: Use stacking as a structured, measurable support—not a hope-based fix
BPC-157 and TB-500 stacking is typically discussed for injury recovery because people aim to support tissue repair through complementary pathways. The most important takeaway from my hands-on experience isn’t a specific “magic dose”—it’s that recovery speed depends on combining any protocol with disciplined rehab, conservative load progression, and measurable milestones.
Next step: Pick an injury milestone (pain-free range, swelling reduction, or functional movement tolerance), track it daily for 7–14 days, and adjust your rehab progression based on results—while treating any peptide approach as a time-bounded, reassessable plan rather than an open-ended commitment.
Discussion