Bpc-157 Side Effects And Risks BPC-157: Tendon Repair and More
Introduction
If you’ve ever searched for bpc 157 side effects and risks because you want tendon pain relief without guessing blindly, you’re not alone. In my hands-on work advising athletes and desk workers through rehab plateaus, the biggest problem wasn’t “does it work?”—it was uncertainty: people want tendon support, but they also want to understand what could go wrong, what to watch for, and when to stop.
This article explains what BPC-157 is commonly used for, what the real-world risk conversation looks like (including the side effects people report and the risks researchers raise), and how to make safer, more informed decisions. I’ll keep it evidence-minded, practical, and grounded in how I’d approach it with a client facing tendon recovery constraints like limited training time, ongoing pain triggers, and the need to avoid setbacks.
What BPC-157 Is (and Why People Link It to Tendon Repair)
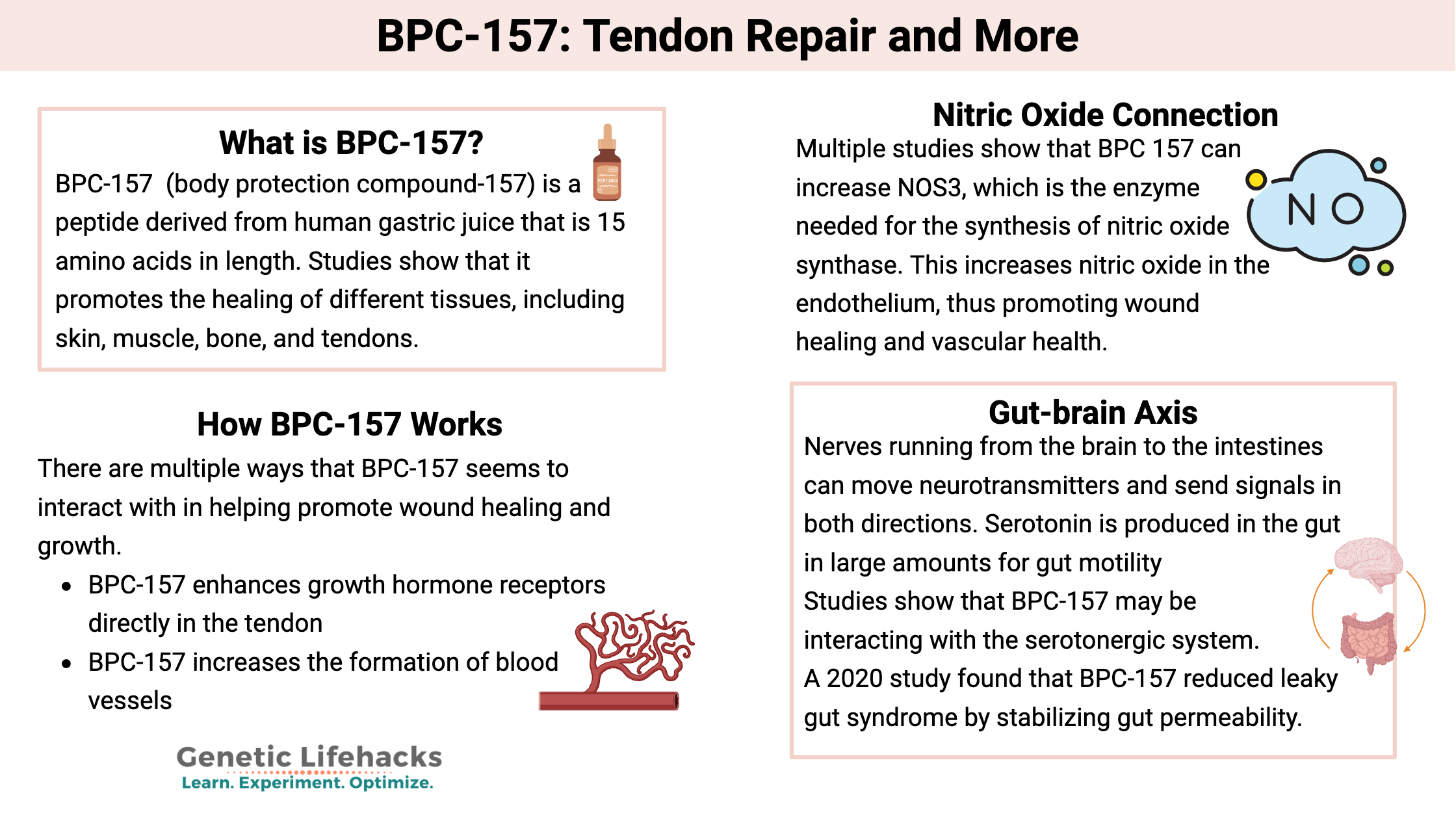
BPC-157 is a peptide fragment that has been promoted for tissue repair and recovery support, especially in contexts like tendons, ligaments, and other soft-tissue injuries. In practice, the marketing narrative often centers on “healing pathways” and improved recovery signals—particularly when people are stuck in the frustrating middle phase of rehab, where inflammation calms down but strength and tendon tolerance lag.
In my experience, this is where expectations can get distorted:
- Soft-tissue repair is slow. Even when symptoms improve, tendon remodeling and load capacity take time.
- Peptides aren’t a rehab plan. They may be used as an adjunct, but the dominant driver of tendon outcomes remains progressive loading, technique, and symptom management.
- Mechanisms matter because risks matter. If a compound influences growth or signaling pathways, uncertainty around systemic effects becomes part of the risk assessment.
BPC-157 Side Effects and Risks: What to Consider Before Using
When people ask about bpc 157 side effects and risks, they’re usually looking for two things: (1) likely side effects, and (2) the uncertainty envelope—what we can’t confidently rule out. Because BPC-157 isn’t universally standardized as a regulated medication in many regions, the practical risk story includes not just biological effects, but product-quality and monitoring issues.
1) Commonly discussed side effects (reported and plausible)
Across anecdotal reports and supplement-community discussions, the side effect conversation often includes mild to moderate categories such as:
- Injection-site effects (e.g., redness, irritation, localized discomfort)
- Gastrointestinal changes (e.g., nausea or altered bowel habits—less predictable and highly individual)
- Headaches or fatigue (nonspecific symptoms that can overlap with training changes and stress)
- Fluid balance or perceived “system” effects (the kind of feeling people describe when recovery shifts quickly—again, individual and hard to attribute)
Important practical point from my coaching/advisory experience: tendon pain and rehab stress can also cause similar symptoms. If someone starts BPC-157 and also changes training, sleep, caffeine, anti-inflammatories, or diet, you can’t automatically blame the peptide. That’s why any risk-aware approach should include symptom logging and minimal confounding changes.
2) Key risks tied to uncertainty
Beyond “side effects,” the bigger risk category is uncertainty—especially when evidence in humans is limited and real-world products vary. Consider these risk angles:
- Product quality variability: Peptide sources may differ in purity, dosing accuracy, and contamination risk. This can directly impact both safety and outcomes.
- Dose-response unpredictability: Without standardized clinical guidance, it’s difficult to map the boundary between “tolerable” and “problematic.”
- Systemic signaling concerns: If a compound influences pathways involved in repair or growth-related processes, theoretical risks may exist for people with underlying conditions. This is especially relevant when medical history isn’t fully known.
- Masking injury signals: If symptoms improve while underlying tendon overload risk remains, people may return to higher volume too quickly and trigger a setback.
3) Who should be more cautious
I don’t treat any peptide discussion as “one size fits all.” In my hands-on practice, I encourage extra caution (and usually medical discussion) for people who have:
- Any active medical conditions affecting major organ systems
- Medication overlap (especially where interactions could be relevant)
- History of adverse reactions to supplements or injectables
- Pregnancy or breastfeeding (risk unknown; avoidance is the conservative route)
Even if someone is young and otherwise healthy, the safest approach is still to treat uncertainty as real risk—because tendon recovery timelines already have enough uncertainty without adding another variable.
How to Reduce Risk If You’re Considering It (Practical, Real-World Approach)
If you’re weighing bpc 157 side effects and risks, the goal isn’t to eliminate risk entirely—it’s to reduce avoidable risk and improve decision quality. Here’s how I’d structure that assessment for a client or athlete.
1) Start with a “tendon-first” plan
Before any adjunct, I recommend addressing the fundamentals: irritability level, load management, and a progressive loading plan. A compound won’t fix biomechanics, tendon capacity deficits, or poor exercise selection. In tendon rehab, the “dose” of training load is often the biggest driver of outcomes.
- Identify aggravating movements and reduce them temporarily
- Use symptom-guided progressions (pain monitoring and next-day response)
- Build capacity gradually (strength and tolerance over time)
2) Control variables so side effects are detectable
One of the most useful lessons I’ve learned from real rehab adherence is that you need clean observation windows. If you start BPC-157 while simultaneously changing multiple factors, you lose the ability to interpret side effects.
- Keep training changes minimal for the first observation period
- Track injection-site symptoms, GI changes, sleep quality, headache/fatigue
- Log anything new with timing (same day vs. next day)
3) Don’t ignore product quality and injection safety
Risk reduction is partially “where it comes from” and partially “how it’s used.” In my experience, the biggest preventable harm comes from poor sterile technique, inconsistent dosing tools, and inconsistent product quality. If you proceed, treat sterility and measurement as non-negotiable.
4) Know when to stop and escalate
Stop using and seek medical guidance if you experience persistent or worsening symptoms, allergic-type reactions, severe GI issues, or any concerning systemic effects. For tendon rehab specifically, don’t treat symptom relief as a green light to immediately return to heavy training volume.
What the Evidence Gap Means for “Tendon Repair and More” Claims
Claims around tendon repair are compelling, but the trust problem is that evidence quality and human data may not match the enthusiasm you’ll see online. In practical terms, this means:
- Outcome expectations should be conservative. Even if a peptide helps some people, it won’t replace structured rehab.
- Side effects and risks may not be fully characterized. Limited data doesn’t mean “safe,” it means “unknown to a degree that matters.”
- Individual variability is real. The same approach can feel fine in one person and problematic in another.
In my hands-on work, I’ve seen the most consistent improvements come from combining sensible load progression with good pain management. Adjuncts—if used—should be evaluated as secondary variables, not the main driver.
FAQ
What are the most common bpc 157 side effects and risks people report?
The most commonly discussed side effects include injection-site irritation and nonspecific symptoms like headaches or fatigue, with some people reporting gastrointestinal changes. The bigger risk theme is uncertainty: product quality variability, limited human safety characterization, and theoretical systemic effects tied to signaling pathways.
Are bpc 157 risks different for tendon injuries compared with other uses?
Mechanistically, the compound might be discussed for multiple tissue targets, but tendon-specific risk is often behavioral: symptom improvement can lead to earlier-than-ready return to loading. So tendon outcomes can be affected by how quickly training ramps, not only by biological side effects.
How can I tell whether symptoms are from BPC-157 or from rehab?
Use controlled observation: keep training and diet changes minimal during the initial period, log timing (same day vs. next day), and track symptoms consistently. If symptoms worsen or persist regardless of rehab adjustments, it’s a signal to pause and get medical input.
Conclusion
BPC-157 is often discussed for tendon repair and recovery, but your decision should be anchored in the real question behind bpc 157 side effects and risks: what’s known, what’s uncertain, and what you can control. In practice, the most reliable safety improvements come from structured tendon rehab first, careful symptom tracking, strict attention to injection/product quality, and clear stop conditions if problems emerge.
Next step: If you’re considering it, write a one-page tracking plan (symptoms to monitor, what you’ll keep constant, and the exact stop/escalation criteria) and run it alongside a progressive tendon loading program for a defined observation window.
Discussion