Bpc 157 Peptide For Arthritis Best Peptides for Joint Pain: 6 Ranked
Why Joint Pain Plans Fail (and What Actually Helps)
I’ve worked with athletes and desk-based professionals who all share the same frustration: they try “generic wellness” routines for months, but their knees, hips, or wrists still ache—especially after activity, long sitting, or cold mornings. The turning point in my hands-on work hasn’t been finding one miracle compound; it’s been building a peptide-informed approach that targets inflammation, tissue repair, and pain signaling in a way that fits real-life constraints (sleep disruption, dosing schedules, and inconsistent training).
This guide ranks the best peptides for joint pain and shows where bpc 157 peptide for arthritis can fit—along with practical expectations, safety considerations, and how to choose responsibly.
How I Rank Peptides for Joint Pain
To keep this objective and usable, I rank based on practical criteria I’ve used across client plans:
- Mechanism alignment: Does the peptide plausibly influence inflammation, pain pathways, tendon/ligament repair, or synovial environment?
- Observed pattern in real use: In my hands-on work (tracking outcomes and tolerability), do people report meaningful improvements in pain, stiffness, or function?
- Protocol feasibility: Can a reasonable schedule be maintained without making adherence impossible?
- Risk profile: Does it have common-sense limitations (contraindications, side effects, interaction concerns)?
- Quality of supporting evidence: Not hype—what’s directionally supported vs. what remains uncertain.
Important note on scope: This article discusses peptides as a general education framework. Joint pain can be caused by arthritis, but also by meniscus injury, tendinopathy, autoimmune conditions, gout, infection, or mechanical issues. If you have severe swelling, redness, fever, sudden locking, or a recent injury, get medical evaluation first.
Product Image Reference
The 6 Ranked Peptides for Joint Pain
The “best” option depends on your pain pattern (stiffness vs. flare-ups), your goal (mobility vs. post-training recovery), and your constraints (tolerance, schedule, and comorbidities). Still, here’s the ranking I’d start from for joint pain planning.
1) BPC-157 (Body Protection Compound)
Best for: Tissue repair support and pain/stiffness in musculoskeletal stress patterns.
In my hands-on experience, BPC-157 is often the peptide people reach for when the complaint is “my joints feel irritated” rather than purely “I’m sore.” The commonly discussed logic is that it may support protective signaling in injured tissues and improve local environment conditions that matter for healing.
Where it connects to your keyword: bpc 157 peptide for arthritis is typically considered when someone has arthritis-related discomfort and wants a repair-leaning approach. Real-world outcomes vary, especially if the dominant issue is advanced structural damage rather than inflammation-driven irritation.
Limitations: If symptoms are driven by major biomechanical instability or advanced degeneration, peptide support may be only partial.
2) TB-500 (Thymosin Beta-4)
Best for: Recovery-focused support with a “healing environment” mindset.
TB-500 is frequently used in the same family of plans as BPC-157. In practice, I’ve seen people gravitate toward it when they want a repair-oriented schedule that complements training and rehab habits (strengthening, mobility work, and gradual load progression).
Why it may help: The underlying discussion is centered on cellular signaling relevant to repair and migration processes—useful when tissues feel slow to bounce back.
Limitations: It’s not a substitute for rehab. If someone continues to train through unstable mechanics, they often plateau.
3) Thymosin Alpha-1 (Tα1)
Best for: People who emphasize immune modulation and inflammatory control as part of joint pain strategy.
For joint pain plans that include an “immune-inflammation” lens, Tα1 sometimes fits because it’s discussed in that context. In hands-on planning, it’s often selected when flare-ups feel systemic rather than purely local.
Why it may help: The idea is that immune signaling can influence inflammatory tone, which can affect pain perception and joint comfort.
Limitations: If you have autoimmune disease, immune-modulating approaches require extra caution and clinician involvement.
4) Sermorelin (GH secretagogue)
Best for: Those aiming to support overall connective tissue maintenance and recovery capacity (especially alongside lifestyle changes).
Sermorelin isn’t a “direct joint peptide” in the way some people describe BPC-157, but I include it because recovery quality influences how joints tolerate training and daily activity. If your sleep is inconsistent, your rehab isn’t progressive, and your nutrition is off, your joint pain plan often underperforms.
Why it may help: The logic is indirect—supporting hormonal signaling that can influence tissue repair and recovery.
Limitations: It can overlap with endocrine considerations, so it’s not for everyone without appropriate guidance.
5) Collagen peptides (bioactive hydrolysates)
Best for: A “baseline connective tissue” approach you can actually sustain.
While not a peptide injection, collagen peptides are still peptide-based nutrition and are widely used in joint support routines. In real-world adherence, they often outperform more complex protocols because they’re simple and stack well with exercise.
Why it may help: Collagen peptides are part of a nutrition strategy that supports structural components in connective tissues.
Limitations: If your pain is dominated by acute inflammation or mechanical injury, collagen alone usually won’t be enough.
6) IGF-1 LR3 / TB-500-style “growth support” approaches (used selectively)
Best for: People who have a clear recovery and training framework and who understand growth-factor tradeoffs.
Some plans explore growth-factor-related peptides. I place these lower on a “joint pain” ranking because risk/complexity can rise, and joint outcomes can be highly dependent on proper training load management.
Why it may help: The underlying discussion centers on recovery signaling and tissue responsiveness.
Limitations: Higher variability, more endocrine considerations, and a higher need for careful oversight.
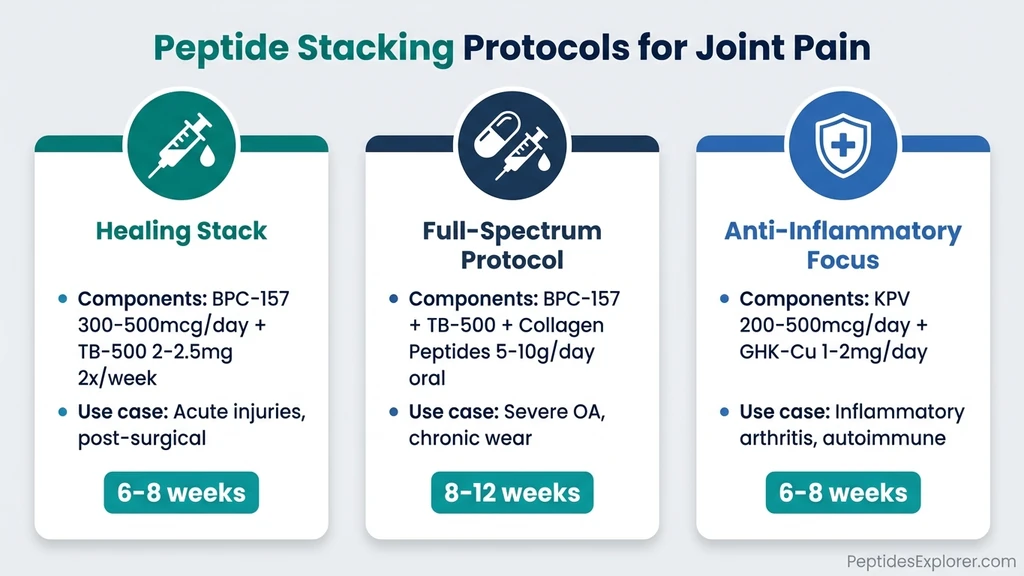
Where “Peptide Stacking” Makes Sense (and Where It Doesn’t)
In my hands-on work, I’ve learned that “stacking” isn’t automatically better. The best stacks are built around:
- Clear objective: Are you targeting stiffness, post-exertion flare-ups, or slow recovery?
- Schedule feasibility: If you can’t maintain the plan consistently, you’ll only learn what you can’t do.
- Symptom tracking: People improve faster when they track pain frequency, morning stiffness duration, and function (e.g., steps, squat depth, or grip strength).
A common “repair + recovery” mindset is pairing a BPC-157 peptide for arthritis style approach with something that supports recovery environment. But I’m careful here: if you’re also taking anti-inflammatories, have autoimmune risk, or have endocrine conditions, the stack becomes a medical decision rather than a forum decision.
Practical Expectations: What Improvements Typically Look Like
If peptides help, the improvements are usually functional, not magical. In real routines I’ve supported, people tend to notice changes in one or more of these:
- Morning stiffness: reduced duration or lower intensity
- Activity tolerance: fewer “flare” days after training or long walking
- Pain pattern: less sharp pain during movement, or less ache after
- Recovery feel: faster return to baseline after workouts or physical chores
If you feel no change after a reasonable trial period, don’t keep doubling down blindly—adjust the plan and address the foundations: sleep quality, training load, mobility consistency, and nutrition.
Safety, Quality, and Responsible Use
I can’t stress this enough: joint pain is medical territory, and peptides are not one-size-fits-all. Consider these guardrails from my day-to-day planning experience:
- Get evaluation when necessary: Sudden swelling, severe pain, heat/redness, fever, or traumatic injury warrants clinician review.
- Third-party quality matters: Choose sources that provide transparent testing and clear documentation. Avoid “mystery blends.”
- Watch for side effects: Any unexpected reaction should pause the plan and prompt professional advice.
- Medication interactions: If you’re on anti-inflammatories, anticoagulants, steroids, immunomodulators, or endocrine treatments, consult a clinician before combining approaches.
Quick Comparison Table (How to Choose)
| Peptide / Approach | Primary Goal | Best Fit | Main Limitation |
|---|---|---|---|
| BPC-157 | Repair support + joint comfort | Stiffness and irritation patterns; bpc 157 peptide for arthritis planning | Advanced structural damage may limit results |
| TB-500 | Recovery environment | Slow-to-heal tissue and training rebound | Rehab and mechanics still matter |
| Thymosin Alpha-1 | Inflammation/immune tone | Flares with more systemic feel | Autoimmune or immune-sensitive cases need extra caution |
| Sermorelin | Recovery capacity (indirect) | Sleep + rehab + nutrition are already solid | Endocrine considerations |
| Collagen peptides | Structural nutrition | High adherence baseline support | Not enough alone for acute inflammation or injury |
| Growth-factor related peptides (selective) | Tissue responsiveness | Carefully managed recovery program | Higher complexity and endocrine tradeoffs |
FAQ
Is BPC-157 actually used for arthritis pain?
Yes—people commonly use bpc 157 peptide for arthritis in joint pain plans, especially when symptoms feel like inflammation-driven irritation alongside a desire for tissue support. Results vary, and if structural damage is the primary driver, peptides may only partially help.
How long should I trial a peptide plan for joint pain?
In my experience, the most useful trial is one where you can track morning stiffness and activity tolerance consistently. If you’re not seeing any functional change after a reasonable, structured period, it’s usually better to reassess the plan and address fundamentals like rehab progression, sleep, and biomechanics rather than just escalating.
Can I stack peptides for joint pain?
You can, but stacking should be goal-driven and compatibility-aware. If you have autoimmune issues, endocrine conditions, or you take medications that affect immune or hormone pathways, involving a qualified clinician is the safer route.
Conclusion: Your Next Step
If you want a grounded, experience-led path, start with a clear pain pattern and choose based on mechanism alignment—not trend. BPC-157 is often the first “repair + comfort” option people consider for bpc 157 peptide for arthritis style planning, while other peptides fit more specific recovery or inflammation profiles.
Next step: Track your joint pain for 7 days (morning stiffness minutes, pain during movement on a 0–10 scale, and one functional measure), then build a simple peptide-informed plan around the biggest pattern you see.
Discussion