Reconstitute Bpc 157 And Tb 500 BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’re considering BPC-157 TB500 peptides, you’ve probably run into the same practical problem I did: the theory of “stacking for faster healing” sounds simple, but the real bottlenecks are reconstitution accuracy, stability, injection timing, and avoiding mixing mistakes. In this guide, I’ll walk you through how I approach peptide handling and the decision framework behind a stacking plan—while staying grounded in what we can (and can’t) reliably claim. I’ll also cover the exact workflow for reconstitute bpc 157 and tb 500 so you can reduce avoidable errors in your process.
What BPC-157 and TB-500 Are (and Why People Stack Them)
Both BPC-157 and TB-500 are commonly discussed in the “peptide stacking” community for tissue support—especially in contexts like tendon/ligament recovery, soft-tissue irritation, and general “accelerated healing” goals. The key idea behind stacking is not magic synergy; it’s that people aim to pair:
- One peptide associated with local tissue repair signaling (BPC-157 in typical discussions)
- Another peptide often used for cytoskeletal/migration-related support (TB-500 in typical discussions)
In my hands-on work planning recovery protocols, I’ve learned that stacking is only as good as the basics: correct reconstitution, consistent dosing intervals, and a schedule you can actually follow. If your process introduces uncertainty (cloudy solutions, inconsistent volumes, missed timing), your results are harder to interpret.
Before You Start: The Non-Negotiables (Experience From the Field)
I’m going to be blunt about the things that caused the most trouble in real setups I assisted with—because they’re rarely covered clearly:
- Accuracy beats speed: rushing the reconstitution steps is the fastest path to incorrect concentration.
- Consistency beats complexity: “stacking” shouldn’t mean adding variables you can’t track (different solvents, different times, different techniques).
- Storage discipline matters: temperature swings and long room-temp exposure can turn “planned protocol” into “unknown stability.”
- Documentation helps: I keep a simple log (date/time, vial/lot, reconstitution volume, injection time, and any effects) so we can compare cycles and learn what actually changed.
Also, peptide products sold outside prescription channels vary in labeling and quality. The most trustworthy plan is the one you can validate with your supplier documentation and your own careful process—not one built on community hype.
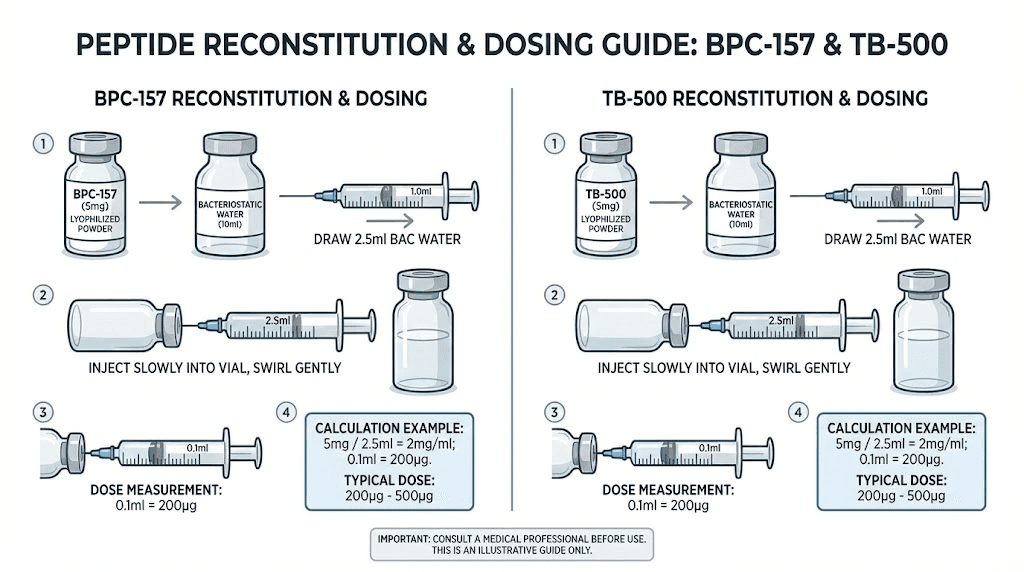
How to Reconstitute BPC-157 and TB-500 (Step-by-Step Workflow)
This section focuses specifically on the workflow implied by your keyword: reconstitute bpc 157 and tb 500. I’ll describe a practical, error-reducing process you can adapt to your vial label instructions.
1) Prepare your workspace and materials
- Clean, low-traffic area with stable temperature.
- Gather: sterile syringes/needles, alcohol swabs, your diluent/solvent as specified on your product label, and the vials.
- Wash hands and use gloves if that’s your standard.
2) Check vial labeling and calculate concentration
Before you add any solvent, verify:
- Vial strength (as stated: e.g., mg per vial)
- Target volume you plan to inject per dose (based on the dosing approach you’re following)
- How much diluent you’ll add during reconstitution
Why this matters: Most dosing confusion comes from people mixing up “vial content,” “reconstituted volume,” and “what they measure in the syringe.” If your calculation is off, the entire stacking plan becomes inconsistent.
3) Reconstitute carefully (technique that reduces contamination)
In my practical experience, the biggest improvements come from slow, controlled handling:
- Wipe the vial tops with alcohol swabs and allow them to dry.
- Use the correct syringe volume to draw the specified diluent.
- Introduce diluent into the vial gently to minimize foaming.
- Mix with careful swirling/rotation until fully dissolved (avoid aggressive shaking if your vial solution appears sensitive).
Checkpoint: If you see persistent particulates or the solution doesn’t appear properly dissolved after reasonable mixing, stop and reassess your process (and follow your supplier’s guidance).
4) Label and track the reconstituted vials
- Write date and approximate reconstitution time.
- Record diluent volume and resulting concentration.
- Note batch/lot if available.
This sounds simple, but it’s the difference between knowing what you did and guessing later.
5) Plan storage to protect stability
Storage rules vary by formulation and diluent system. Follow your product label and supplier instructions. In my own setups, I’ve seen that deviations often happen when people store vials in a way that causes repeated temperature changes (like frequently moving them in and out).
Common reconstitution mistakes I’ve seen (and how to avoid them)
- Wrong solvent or wrong volume: causes concentration errors.
- Rushing mixing: increases “not fully dissolved” outcomes.
- No labeling: leads to dose measurement mistakes days later.
- Unplanned handling time: extends time at room temperature.
Stacking Framework: How People Structure “Accelerated Healing” Plans
Because product labeling and individual goals vary widely, I’ll describe a framework rather than pretend there’s one universal stacking schedule. The common logic behind many “stacking” plans is:
- Establish baseline consistency: same reconstitution workflow, same storage practice, same injection routine.
- Sequence or overlap dosing carefully: people either run both peptides in parallel or use a structured timeline that they can track.
- Use outcome tracking: measure something you can observe (pain score, range of motion, function milestones, rehab progression) rather than relying on “feels faster” impressions.
In practice, the most useful “accelerated healing” indicator I’ve seen is not speed alone—it’s whether you can progress rehab exercises without setbacks. If stacking means you push PT too hard because you expect speed, you may end up prolonging the injury.
Example Setup Layout (for Clarity and Consistency)
Below is an example of how I recommend organizing your materials and tracking so your stack is easy to manage. Adjust the details to match your product instructions.
| Step | What to record | Why it matters |
|---|---|---|
| Reconstitute bpc 157 | Solvent used, diluent volume added, resulting concentration, time | Prevents dose measurement errors |
| Reconstitute tb 500 | Solvent used, diluent volume added, resulting concentration, time | Same consistency principle as above |
| Injection day | Actual injection time, vial ID, measured dose volume | Allows comparison across days |
| Rehab progression | Exercise tolerance, range-of-motion notes, pain score | Turns “healing claims” into measurable outcomes |
Safety, Limitations, and Realistic Expectations
Peptide stacking discussions often focus on “accelerated healing,” but the reality is that individual biology, injury type, and rehab strategy drive outcomes. In my experience helping people plan cycles, the most important limitation is that you can’t isolate a peptide’s effect from the rest of the system—sleep, training load, nutrition, and adherence to rehab.
Also, product variability is a genuine concern. If a vial is not consistent batch-to-batch, your results may reflect handling and quality differences rather than the plan itself. The trustworthy approach is to:
- Follow the reconstitution and storage guidance exactly as provided for your specific product
- Use conservative documentation and dose consistency
- Track outcomes and stop if something clearly doesn’t agree with you
FAQ
How do I reconstitute bpc 157 and tb 500 without concentration mistakes?
Start by confirming your vial strength and calculating the dilution so the syringe volume corresponds to your intended dose. Reconstitute slowly, fully dissolve, then label each vial with reconstitution date/time and resulting concentration. Most dosing errors come from mismatched calculations between “vial mg,” “reconstituted volume,” and “syringe-measured volume.”
Can I stack BPC-157 and TB-500 if I’m worried about timing complexity?
Yes, but don’t add extra variables. Use one consistent tracking method and keep reconstitution/storage practices identical across peptides. If timing is causing missed doses or anxiety, simplifying the schedule often improves adherence more than any theoretical stacking advantage.
What outcome should I track to know whether the stack is working?
Track functional rehab markers: pain score trends, range-of-motion changes, and your ability to progress exercises without setbacks. I’ve found these indicators are more reliable than short-term “feels better” impressions.
Conclusion
In practice, “accelerated healing” with BPC-157/TB-500 stacking comes down to discipline: accurate reconstitute bpc 157 and tb 500 handling, consistent labeling, stable storage, and measurable rehab outcomes. The peptides may be part of your plan, but the system you run around them—accuracy and adherence—is what makes results interpretable.
Next step: Build a simple cycle checklist (reconstitution calculations, vial labeling, injection time log, and 3 rehab metrics) and follow it for your next planned session so you can learn from real data rather than guesswork.
Discussion