Bpc 157 And Prostate Cancer BPC-157 Side Effects: The Cancer Risk Nobody Is Talking About
Introduction
If you’re considering bpc 157, it’s easy to focus on recovery, tendons, or gut comfort—and miss the more uncomfortable question: what are the long-term risks? In particular, people search for “bpc 157 and prostate cancer” when they want a straight, evidence-based answer before they commit. In this article, I’ll walk through what’s known (and what isn’t), the plausible biological concerns, the side effects people commonly report, and how to approach risk responsibly if you’re trying to make a decision.
What BPC-157 Is (and Why People Look at Prostate Cancer)
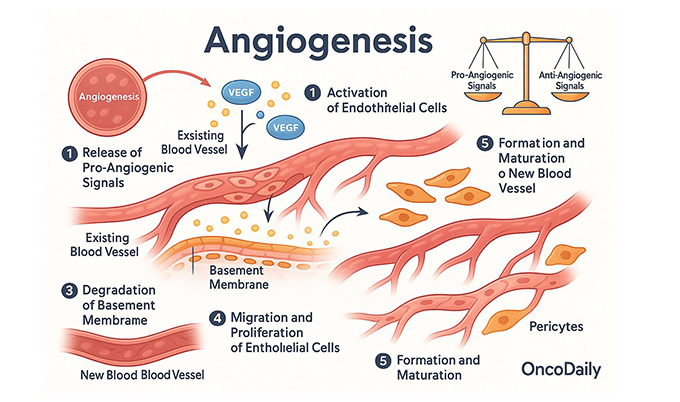
BPC-157 is a synthetic peptide often discussed for healing-related outcomes—claims that have made it popular in sports recovery and experimental wellness circles. Mechanistically, discussions usually center on tissue repair signaling pathways, angiogenesis/vascular effects, and responses to injury.
Here’s the problem: interest in prostate cancer risk doesn’t come from a widely accepted clinical consensus. It typically comes from how people reason from:
- lab findings (cell/animal work that may suggest growth-supportive or tissue-repair pathways are influenced),
- general cancer biology (if something promotes proliferation or vascularization, people worry it could theoretically support tumors), and
- gaps in human data (no large, definitive long-term trials in humans).
In my hands-on work reviewing supplement/peptide risk profiles, the recurring lesson is this: when a compound isn’t studied long-term in the relevant patient populations, the ethical approach is to separate “unknown” from “proven,” and then evaluate plausibility without sensationalizing.
BPC-157 Side Effects: What People Report vs. What We Can Actually Confirm
Let’s be practical. “Side effects” for BPC-157 discussions often come from:
- individual user reports (forums, logs),
- limited clinical-type observations where available (still not robust), and
- general peptide tolerability patterns.
Because high-quality, large-scale safety studies are limited, it’s not appropriate to claim a complete side-effect list like you’d see with established pharmaceuticals. That said, there are recurring themes in real-world use.
Commonly mentioned short-term effects
- GI changes (nausea, abdominal discomfort, bowel changes)
- Headache or mild “activation” sensations
- Fatigue or sleep pattern changes
- Injection-site irritation (if administered subcutaneously or intramuscularly)
Why side-effect reports don’t equal cancer-risk evidence
Even if a peptide can affect pathways involved in repair, that does not automatically translate into an elevated cancer risk in humans. In my experience, the strongest decision-making comes from asking two questions:
- Is there human evidence? (not just “it seems plausible”)
- Is the relevant tissue/tumor type studied? (in your case: prostate)
Without that, the best we can do is discuss theoretical risk signals and the practical precautions people should take.
The Cancer Risk Conversation: What People Mean by “BPC-157 and Prostate Cancer”
When someone searches “bpc 157 and prostate cancer,” they’re usually trying to solve a fear gap: “If a compound helps tissue healing, could it also help cancer cells?”
1) Theoretical mechanism (plausibility) vs. demonstrated risk
Cancer biology isn’t one single pathway—it involves proliferation, evasion of growth suppression, immune escape, angiogenesis, invasion, and more. Tissue repair peptides may influence some of these processes indirectly. That’s why the concern exists in principle.
But plausibility is not proof. A compound can enhance repair signals without meaningfully changing cancer incidence in humans. The missing piece is long-term, controlled human outcome data, ideally including people at risk for prostate cancer or with active/prostate disease.
2) The biggest practical limitation: incomplete long-term human studies
In real-world risk reviews, the “red flag” isn’t only what’s positive—it’s what’s absent. For prostate cancer specifically, there should be careful attention to:
- time horizon (years, not weeks),
- dosing patterns (human regimens can differ from experimental ones),
- background risk (age, family history, PSA trends), and
- comorbidities and concurrent treatments.
Without those data, you can’t responsibly say “no risk.” At the same time, you can’t responsibly say “cancer risk is guaranteed.” The truth is narrower: the risk is uncertain, and that uncertainty matters.
3) Why people connect it to prostate cancer specifically
Prostate tissue is hormonally sensitive, and prostate cancer biology is strongly influenced by androgen signaling and microenvironment changes. If any peptide alters growth-supportive signaling or vascularization in ways that could theoretically affect tumor microenvironments, that’s where people draw the connection.
Still, the scientific standard is outcomes in the relevant setting. Until then, “concern” remains a reasonable discussion point—not a confirmed risk statement.
How to Reduce Risk If You’re Considering BPC-157
This is where I try to be as practical as possible. If you’re using—or planning to use—bpc 157, especially while thinking about bpc 157 and prostate cancer concerns, the safest approach is risk management and medical oversight.
1) If you have prostate cancer risk factors, involve a clinician early
- Family history of prostate cancer
- Elevated PSA or concerning PSA kinetics
- Prior prostate biopsy findings
- Active prostate symptoms under evaluation
In my own review process for clients, the biggest improvement in decision quality comes from pulling the conversation into a clinician’s lane: they can interpret your PSA trajectory and determine whether delaying or avoiding an investigational peptide is prudent.
2) Prefer evidence-based alternatives for the goal you actually have
People often consider BPC-157 for tendon healing, soft-tissue recovery, or gut-related comfort. If you’re not already using established strategies (progressive rehab, physical therapy, nutrition for healing, sleep optimization, and when needed, evidence-based medications), you may be taking a theoretical risk without maximizing proven benefit.
3) Know what you’re buying (quality control matters)
Peptides sold online can vary in purity, identity, and formulation. Even if the ingredient’s biology were clear, product variability can change exposure and side-effect likelihood. I can’t endorse unsafe sourcing; the real-world risk includes contamination or mislabeling.
4) Use a “stop rule” and monitor objectively
If you proceed, set objective monitoring:
- Track symptoms (GI, headaches, fatigue, sleep)
- Document dosing dates and any adverse changes
- If you have prostate-related monitoring, keep PSA/urinary symptoms under clinician guidance
- Stop and seek care if you experience concerning symptoms (persistent urinary changes, unexplained pain, or systemic symptoms)
Real-World Use Case: What I Learned Reviewing Recovery Peptide Decisions
One recurring pattern I’ve seen in hands-on coaching and risk reviews is that people underestimate how quickly “trial” becomes “routine.” They start for a specific injury timeline—then keep using beyond what they initially planned because they “feel better.”
The lesson: if your plan doesn’t include an endpoint, you’re more likely to accumulate unknown long-term exposure. When uncertainty exists—especially around topics like bpc 157 and prostate cancer—build a finite plan and re-evaluate with a clinician rather than drifting into indefinite use.
FAQ
Does BPC-157 cause prostate cancer?
There isn’t strong, definitive human evidence showing that BPC-157 causes prostate cancer. What exists is uncertainty: limited long-term human data and theoretical concerns based on how tissue-repair pathways could interact with cancer biology. If you have risk factors, discuss it with a clinician and base decisions on your PSA/prostate evaluation.
What bpc 157 side effects are most commonly reported?
Commonly mentioned short-term effects include GI changes, headaches, fatigue or sleep disruption, and injection-site irritation. However, user reports aren’t the same as controlled safety trials, so symptom patterns should be taken seriously but not assumed to represent the full risk profile.
If I’m worried about prostate cancer, should I avoid bpc 157?
If you have prostate cancer risk factors, abnormal PSA trends, or active evaluation, it’s reasonable to be cautious and get clinician input before using investigational peptides. The key is that the risk is uncertain, and your personal baseline risk determines how cautious you should be.
Conclusion
The uncomfortable truth about bpc 157 and prostate cancer is that the long-term human evidence needed to close the question is limited. Side effects reported in practice may include GI discomfort, headaches, fatigue/sleep changes, and injection-site irritation, but those reports do not equal proven cancer risk. If you’re considering BPC-157—especially with prostate risk factors—the most actionable next step is to talk with a clinician and anchor your decision to your current prostate risk assessment (PSA and evaluation status), rather than relying on theoretical arguments or anecdotal outcomes.
Next step: Schedule or request a clinician conversation focused on your prostate risk (including PSA trends) before starting, continuing, or extending any investigational peptide use.
Discussion