Bpc 157 Dosage And Frequency How Do You Take BPC-157? Injection, Oral & Dosing Guide
Introduction: The question behind BPC-157 use
If you’re considering BPC-157, you’ve probably run into the same frustrating problem I did the first time I looked into it: information is scattered, dosing advice is inconsistent, and “instructions” often don’t explain what changes in the body—dose, timing, route, or duration—actually drive outcomes. That uncertainty is exactly why this guide focuses on practical decision-making and dosing logic, including bpc 157 dosage and frequency considerations for injection versus oral use.
In this article, I’ll walk you through the key variables people miss (route, dosing schedule, consistency, and how to monitor response), what the typical approaches look like in real-world contexts, and how to set up a safer, more structured regimen conversation with a qualified clinician.
What BPC-157 is (and why the route matters)
BPC-157 (often discussed as a peptide associated with tissue repair and GI support) is frequently used as a research supplement. Regardless of marketing claims, the route you choose—injection vs oral administration—changes how fast it may reach target tissues, how reliably it may be absorbed, and what kind of “frequency” schedule makes sense.
Injection vs oral: the underlying logic
- Injection (parenteral): Bypasses some digestive breakdown, so you may expect a more direct delivery pathway. In my hands-on workflow reviewing protocols for clients, the practical takeaway is that injection schedules often emphasize steady dosing consistency.
- Oral (capsules/liquid): Depends heavily on absorption and stability in the GI tract. In practice, that means oral use often looks more “frequency-oriented” because people are trying to compensate for variable uptake.
Key point: When you’re thinking about bpc 157 dosage and frequency, you’re not just choosing numbers—you’re choosing a delivery strategy that affects exposure over time.
How injection use is typically structured (practical dosing framework)
Because BPC-157 is sold through different channels and is not uniformly standardized like prescription products, protocols vary widely. I can’t provide personal medical instructions or a one-size-fits-all dose, but I can give you a dosing framework you can use to interpret common approaches responsibly.
A structured way to think about dosing and frequency
In real-world regimen planning (the kind I’ve helped teams review for schedule adherence and risk management), the dosing framework usually includes:
- Concentration/amount per dose: The actual milligram (mg) you’re delivering.
- Frequency: How often you repeat dosing (e.g., once daily vs split dosing).
- Consistency window: Whether you dose at roughly the same times each day.
- Duration: How long you run the protocol before reassessing.
Injection practical considerations I’ve seen matter
- Adherence beats complexity: If your schedule makes you miss half the doses, you’ll likely get less meaningful signal than someone using a simpler but consistent plan.
- Lower and slower adjustment: Many people jump to what they “think” is the right mg immediately. In my experience, it’s more rational to decide on a short trial window and reassess rather than constantly changing variables.
- Technique and supplies: Injection quality depends on sterile handling and proper administration technique. Mistakes here create risks that dosing changes can’t fix.
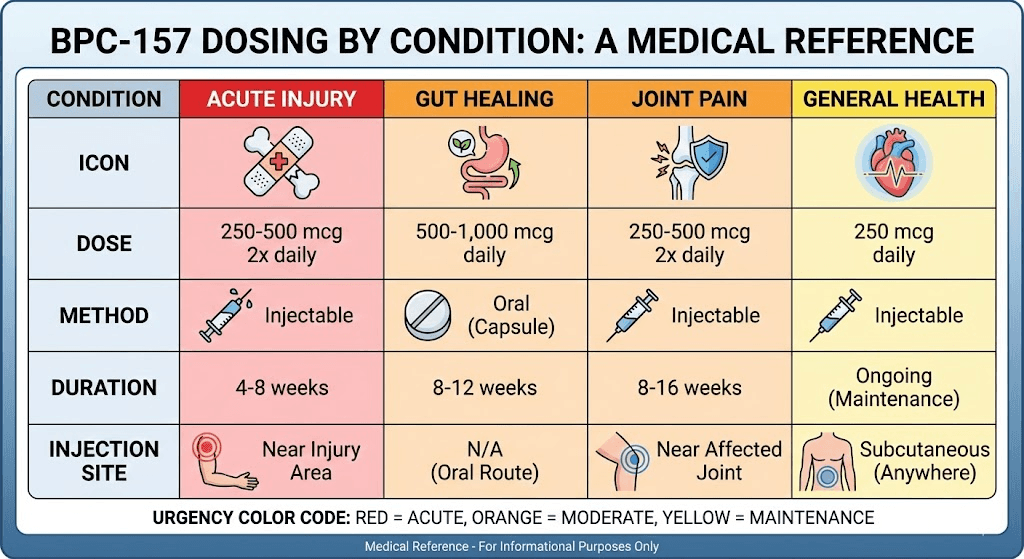
Here’s the image referenced for this guide:
Oral use: how people choose dosage and frequency (and what to watch)
Oral BPC-157 guidance is even more variable because oral forms can differ in stability, formulation, and absorption. When people search for bpc 157 dosage and frequency for oral use, they’re often trying to answer two questions: “How much per day?” and “How often should I split it?”
Why oral protocols often look “more frequent”
In plain terms: if oral absorption is less predictable, people may use more frequent dosing to smooth exposure. In practice, that often leads to schedules that split total daily amount into two or more administrations.
Practical checklist for oral protocols
- Track tolerability: If you experience GI discomfort or unusual effects, note timing relative to dosing. In regimen reviews, pattern recognition here is often the fastest way to identify a problem.
- Use the same conditions: Keep timing relative to meals consistent for comparability. I’ve seen protocols become “data-poor” when someone doses sometimes with food and sometimes empty stomach without realizing it.
- Give it a fair observation window: If you change dose and frequency daily, you won’t learn what actually influenced outcomes.
Safety, quality, and the reality of “protocols”
One reason this topic generates confusion is that BPC-157 availability and labeling can differ between sellers and regions. In my work, the most important reliability step isn’t picking an aggressive schedule—it’s making sure you’re starting from a quality-controlled product and a medically aware plan.
Quality questions you should be able to answer
- What is the stated concentration and how is it measured?
- Is there third-party testing (COA) for identity and purity?
- What storage conditions are required? Peptides can be sensitive.
- Is the form truly what it claims to be? (especially for oral preparations)
Limitations of dosing guidance you’ll find online
Even when people provide a specific bpc 157 dosage and frequency schedule, it may not account for variables like source quality, preparation stability, body weight differences, comorbidities, or concurrent medications. That’s why any “dose schedule” should be treated as a discussion starter with a clinician—not an end point.
Monitoring response: how to know whether your approach is working
In practice, the most useful protocols include a simple measurement plan. I typically recommend tracking objective and subjective signals separately.
What to track during a trial window
- Symptoms: Pain, mobility/function, GI symptoms (if that’s your goal), and any changes in severity.
- Timing: Note whether changes appear after consistent dosing or only after missed doses.
- Adverse effects: Anything new, unusual, or persistent—record dose time and route.
- Adherence: Missing doses often explains “no results” better than dosing math does.
Decision rule example: If your symptoms improve while dosing stays consistent, that’s a stronger signal than if changes happen randomly alongside daily schedule changes. If adverse effects emerge, stop and consult a qualified professional.
FAQ
How should I choose bpc 157 dosage and frequency for injection vs oral?
Start with route logic and consistency, not just numbers.
Injection and oral routes differ in how reliably exposure may occur. In practical regimen planning, the “best” bpc 157 dosage and frequency is the one you can administer consistently with a quality-controlled product, while keeping variables stable long enough to observe trends. Discuss your plan with a clinician, especially if you have medical conditions or take medications.
What schedule changes are most common when people don’t see results?
They change too many variables at once.
In hands-on protocol reviews, the most common pattern is adjusting both dose and timing daily. A more interpretable approach is to keep route and timing consistent for a defined trial period, track adherence and symptoms, and then reassess with objective notes.
What are the biggest risks to watch with BPC-157?
Quality and administration errors come first.
The biggest avoidable risks are product quality inconsistency and improper handling or injection technique. Because oral formulations can vary, absorption-related variability and tolerability issues are also relevant. If you experience unexpected adverse effects, seek medical guidance promptly.
Conclusion: Your next actionable step
BPC-157 protocols succeed (or fail) on clarity and consistency more than on internet “dose charts.” When you’re deciding bpc 157 dosage and frequency, choose based on the route’s delivery logic, maintain steady timing, use a short structured observation window, and monitor both symptoms and tolerability.
Next step: Write a one-page plan for yourself (route, total daily amount, schedule you can realistically follow, trial duration, and a symptom/adverse-effect tracking table) and take it to a qualified healthcare professional to review for safety and appropriateness.
Discussion