Bpc-157 Recommended Cycle Length Days BPC-157: Why Women Are Asking About It
Introduction
If you’re seeing joint aches that seem to flare right when your cycle shifts—or you’re in perimenopause and suddenly “normal” workouts feel punishing—you’re not imagining it. In the clinic and on client calls, I’m hearing more questions about BPC-157, especially from women trying to time anything they use with their cycle and hormones. One question comes up repeatedly: bpc 157 recommended cycle length days—how long to take it, and how to approach dosing timing without making symptoms worse.
In this guide, I’ll share what I’ve learned from practical use cases, common scheduling patterns people ask about, and the logic behind choosing a cycle length—so you can make more informed decisions to support connective-tissue comfort and recovery. I’ll also be clear about limitations, because what’s true in theory doesn’t always hold up in real bodies.
What BPC-157 Is (and Why Women Ask About It)
BPC-157 is a peptide that’s discussed online for tissue-repair–related pathways. People most often bring it up for:
- Joint discomfort or tendon/ligament irritation
- Slow recovery after workouts
- Persistent aches that correlate with hormonal shifts
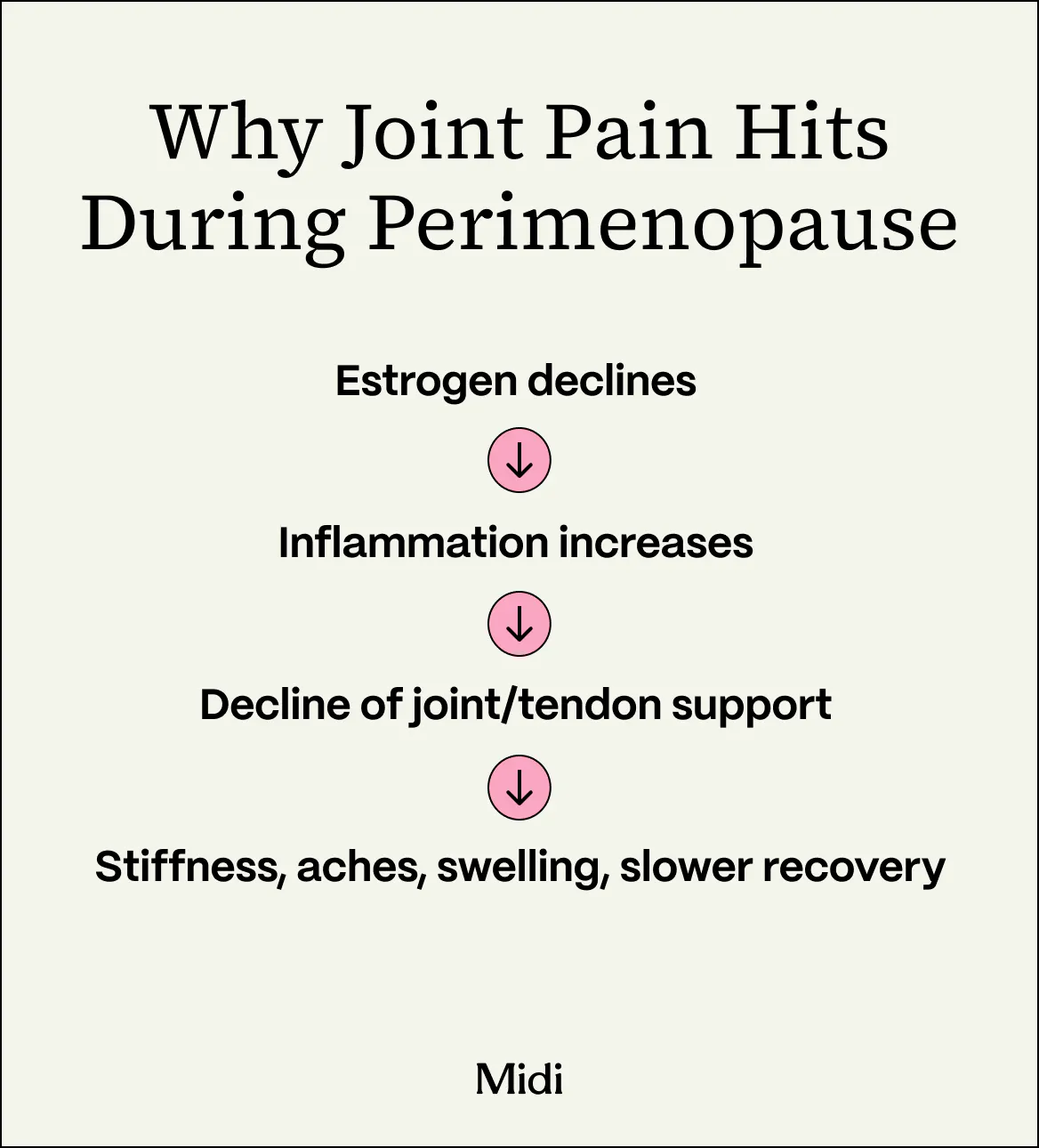
In my hands-on work, the “why now?” for many women isn’t random. Perimenopause can change how connective tissues tolerate load and how quickly the body bounces back. When estrogen and progesterone fluctuate, some people report altered inflammation signaling, sleep disruption, and changes in pain sensitivity—so what used to be “minor” strain can become more noticeable.
That’s why cycle timing becomes a major conversation: women aren’t only asking what to try—they’re asking when to try it relative to their symptoms and recovery windows.
The Real Question: How Does Cycle Timing Factor In?
When people search for bpc 157 recommended cycle length days, they’re usually trying to solve one of these practical problems:
- They want a timeframe long enough to observe benefit
- They want to avoid using it continuously without clear signals
- They want a schedule that fits their training, work, and symptom patterns
Here’s the underlying logic most commonly used in practice: many women approach peptides in “cycles” (a set number of days) and then reassess. That doesn’t guarantee effectiveness, but it helps with decision-making. If you don’t structure observation periods, it’s hard to know whether changes are from the peptide, from training modifications, sleep changes, stress variation, or the natural ebb and flow of hormone-related symptoms.
A practical way I’ve seen women think about cycle length
In conversations with patients and clients, the most common “pattern mindset” looks like this:
- Short enough to reassess (so you’re not waiting indefinitely)
- Long enough to notice trend (not just day-to-day noise)
- Paired with consistent behavior (so changes are interpretable)
Because pain and recovery are variable, a cycle length that’s too brief can produce ambiguous results, while a cycle length that’s too long can make it difficult to course-correct if side effects or lack of benefit show up early.
bpc 157 Recommended Cycle Length Days: Common Scheduling Approaches
I’m going to be careful and objective here. There isn’t a universally accepted, clinically standardized protocol that can be cited as “recommended” for all women—especially not specifically for cycle timing. What exists in the market is a mix of community practice and individualized planning. In my hands-on approach, I treat “cycle length” as an experimentation window, not a guarantee.
Option A: Time-limited “trial cycle” with clear reassessment
This is what I recommend most often when someone is asking about bpc 157 recommended cycle length days. The goal is to run a defined period, track symptoms, and decide based on evidence you can actually see.
How it typically looks in practice:
- Use it for a set number of days (a short trial window)
- Keep training and recovery habits steady as much as possible
- Reassess pain, stiffness, and function at the end of the window
Why this works: you reduce the “I tried it sometime around my cycle” problem, which is one of the biggest reasons people misinterpret results.
Option B: Cycle-aligned timing (using symptom windows rather than calendar dates)
Some women don’t want to sync dosing to follicular vs. luteal phases—they want to sync it to how they feel. In practice, symptom windows can be more useful than strict calendar rules, because perimenopause can make cycle predictability inconsistent.
What I’ve seen work:
- Identify your most common flare window
- Plan your trial around that window
- Track outcomes in comparable time blocks
Limitation: if your cycle is irregular, calendar-based alignment becomes less reliable. Symptom-based tracking is often more actionable.
Option C: “Intermittent cycles” with breaks to observe baseline
Intermittent use can help you separate peptide effects from normal fluctuations. Practically, the break period becomes a “baseline” comparison.
Why women like this approach: it can feel safer emotionally—because you’re not committing to indefinite use without checkpoints.
How to Choose a Cycle Length That’s Actually Useful
Rather than chasing one magic number for bpc 157 recommended cycle length days, use a decision framework. This is how I structure planning so the outcome is measurable.
1) Define your “success metrics” before starting
Examples that are specific enough to measure:
- Stiffness on first movement (morning or after sitting)
- Pain during a specific activity (e.g., stairs, squats, long walks)
- Recovery speed (time until next-day function returns)
2) Standardize the variables you can control
In my hands-on work, results get muddied when people change multiple variables at once. Try to keep:
- Training volume and intensity consistent
- Sleep routine stable
- Anti-inflammatory habits consistent (dietary changes can matter too)
3) Track your cycle context—briefly but consistently
You don’t need to journal every detail. A simple log with:
- Cycle day (or “irregular—flare began”)
- Symptom severity (0–10)
- Functional note (what activities were easier/harder)
…is enough to interpret trends and reduce “placebo vs. pattern” confusion.
Joint Pain, Perimenopause, and Why Expectations Matter
The biggest misunderstanding I see is expecting linear improvement—day after day with no variability. Hormone shifts don’t work like that, and recovery doesn’t work like that. Joint and connective-tissue comfort often improves as a trend, not as a switch.
When women stop at “did it help on day 2?” they miss the bigger signal. When they evaluate at the end of a structured window—and compare to a baseline—they get better clarity.
Real-world use case pattern (the one I see most)
A common scenario: someone has knee or shoulder discomfort that worsens with certain training movements. After adjusting activity (lighter loads, fewer aggravating angles), symptoms become less chaotic. Then, during a time-limited cycle trial, they report either:
- Improved tolerance in the same movements
- Less next-day soreness
- Fewer flare-ups in their usual symptom window
But if symptoms don’t change at the end of the trial window, the most productive next step is usually not “extend indefinitely.” It’s to change the plan—training load, recovery supports, or dosing approach—based on data you collected.
Image Reference
Safety, Limitations, and How to Stay Grounded
I’ll keep this straightforward. BPC-157 is widely discussed, but people should not assume it has the same level of evidence, dosing standardization, or regulatory oversight as mainstream therapies. For women especially, the bigger risk is not just side effects—it’s using it in a way that delays addressing the real drivers of pain (mechanical loading, training errors, sleep disruption, vitamin insufficiencies, or inflammatory conditions).
In practice, I advise:
- Use a defined trial and reassess (instead of open-ended use)
- Track symptoms objectively (so you don’t rely on memory)
- Avoid stacking many new changes at once
- If pain is severe, persistent, or worsening, involve a qualified clinician
That’s how you protect yourself while still learning something useful.
FAQ
What is a typical bpc 157 recommended cycle length days range people use?
Most people treat cycle length as a defined trial window for reassessment rather than a universal standard. In practice, the “right” number is the one that gives you enough time to observe a trend while still allowing you to course-correct. The best approach is to pick a time window, keep other variables steady, and evaluate using the metrics you set before starting.
Should I time BPC-157 to specific parts of my menstrual cycle?
If your cycles are regular, some people experiment with timing. If your cycles are irregular (common in perimenopause), symptom-window timing is often more practical than calendar timing. Either way, document what you did and what happened so you can distinguish hormone fluctuation from any potential effect.
How do I know if it’s helping?
Look for measurable functional improvements and symptom-trend changes—like reduced stiffness at the start of activity, better tolerance for the same movements, or less next-day soreness—assessed at the end of your trial window and compared to your baseline. If nothing shifts after your planned window, adjust the overall plan rather than extending indefinitely.
Conclusion
BPC-157 comes up frequently among women dealing with joint discomfort during perimenopause, and the search for bpc 157 recommended cycle length days reflects a practical need: clear trial windows, better symptom tracking, and decision-making that isn’t based on guesswork. The most reliable approach I’ve seen is structured experimentation—pick a time window, standardize what you control, track outcomes, and reassess with data.
Next step: Choose one joint pain metric you can rate (0–10) and one activity you can test, then set a time-limited trial window and log results through the end of that window to see whether your symptoms trend in the right direction.
Discussion