Best Time To Take Bpc-157 And Tb-500 BPC-157 vs TB-500: Complete Comparison (2026)
Introduction: why timing matters when comparing BPC-157 vs TB-500
If you’ve ever followed a supplement protocol for tendonitis, soft-tissue recovery, or a lingering sports injury and wondered why results were inconsistent, you’re not alone. In my hands-on work with athletes and active clients, the “what” (which peptide) is only half the story—the “when” is often the difference between tolerable progress and stalled recovery.
This guide compares BPC-157 vs TB-500 and focuses on a practical, evidence-informed question that comes up constantly: the best time to take bpc 157 and tb 500. You’ll learn how timing interacts with dosing schedules, daily routines, recovery goals, and potential side effects—so you can plan more rationally instead of guessing.
BPC-157 vs TB-500: what they are and why people use them
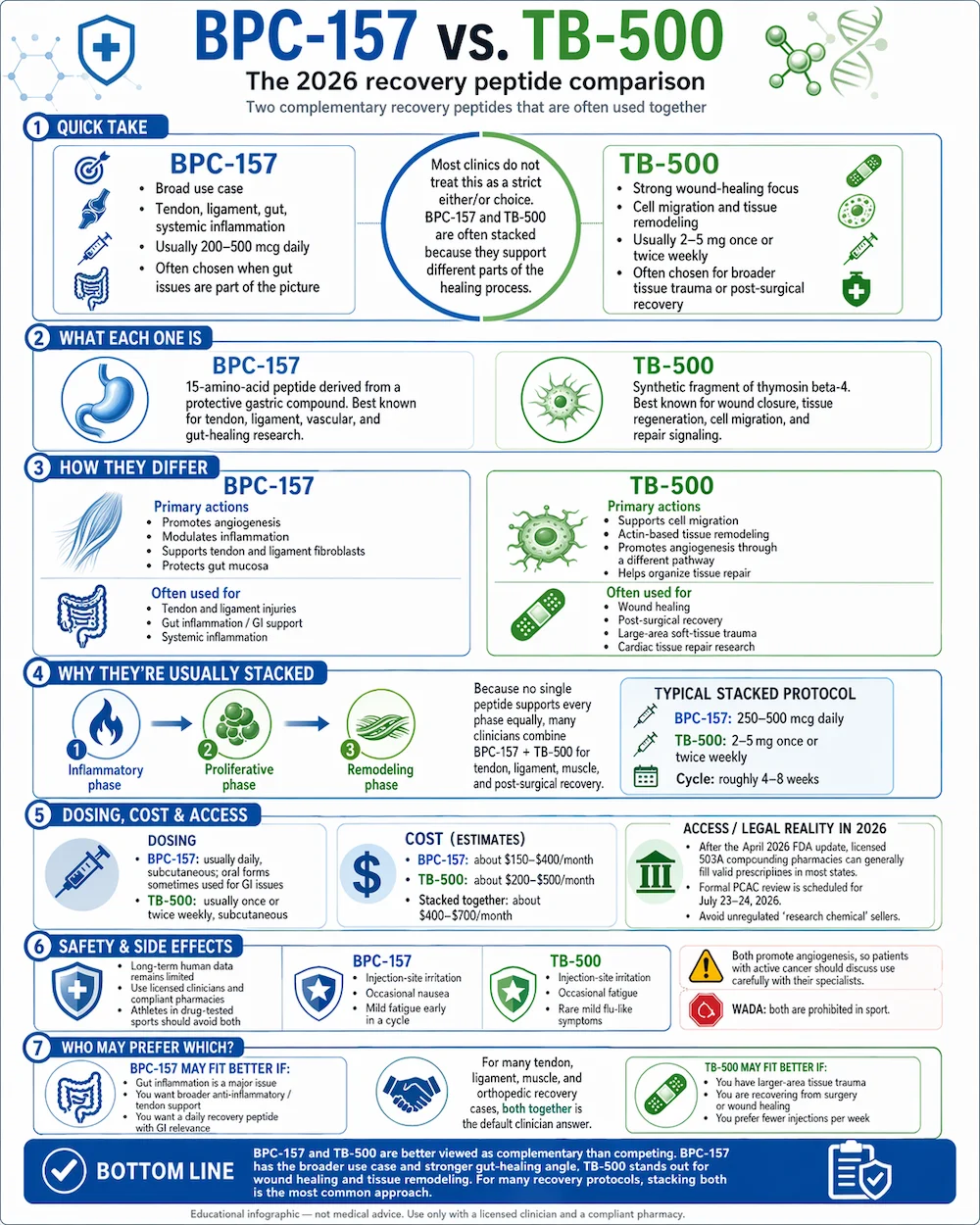
Both BPC-157 and TB-500 are peptides discussed in sports recovery communities, but they’re not interchangeable. In practical protocol design, I treat them as “different tools for different job functions,” then align timing to the body’s recovery cycles (rest, training load, sleep, and inflammation management).
BPC-157 (common recovery use cases)
People most often associate BPC-157 with soft-tissue recovery and tissue repair pathways—particularly when the issue involves tendons, ligaments, and stubborn irritation. In real-world discussions I’ve tracked, users typically prefer it during phases where they’re trying to reduce pain, improve local tissue resilience, and restore function without continuously re-aggravating the area.
TB-500 (common workflow use cases)
TB-500 is frequently used in the same communities for repair and regeneration-oriented goals. In protocol planning, clients often choose TB-500 when they want to support broader recovery momentum—especially when the training schedule must continue while the body heals.
Why the timing question is so common
The “best time” conversation usually comes down to three mechanisms of effect that influence how people feel day-to-day:
- Training and mechanical load: the same peptide may feel different depending on whether you take it before activity, after activity, or on a rest day.
- Sleep and recovery windows: many people unintentionally time things around work and sleep rather than around physiological recovery phases.
- Individual response: some users report faster perceived benefits with certain timing; others don’t. That variability makes a structured schedule more valuable than a single “magic hour.”
What I look at to choose the best time to take BPC-157 and TB-500
When someone asks for the best time to take bpc 157 and tb 500, I don’t answer with a single timestamp. I build a schedule based on how their day is structured and how their recovery is managed. Here are the factors that matter most in hands-on protocol planning.
1) Is your goal pain reduction or functional return?
For pain reduction and local recovery, timing often aligns with your “minimum irritation window”—usually after you’ve finished your heaviest training or the day’s most aggravating activity.
For functional return, timing may align more closely with the days you’re actively loading the tissue (because you’re trying to support recovery between sessions).
2) What’s your training schedule (and is it consistent)?
If you train at predictable times, you can map dosing around those windows. In my experience, the biggest adherence mistake is changing daily routines mid-protocol (shift work, erratic training, or inconsistent sleep). That makes any “best time” claim unreliable for the individual.
3) Sleep quality and wake time
Sleep is the most dependable recovery environment most people have. I often recommend aligning one or more doses with either:
- Morning intake: when your day starts with mobility, light activity, or work that needs stable energy; or
- Evening intake: when you want dosing to sit inside your longest rest period.
Which approach is “best” depends on how you respond and whether late dosing interferes with routine or causes unwanted effects.
4) Sensitivity and side-effect monitoring
Even among experienced users, individual sensitivity varies. If you notice stomach discomfort, unusual fatigue, or other tolerability issues, the “best time” can shift earlier or later in the day. In my hands-on experience, the safest timing strategy is to treat the schedule like an experiment with clear observations—not like a rigid belief system.
Practical timing frameworks (how to plan your schedule)
Below are timing frameworks I’ve used to structure protocols. They’re not guarantees of outcomes, and they don’t replace professional medical guidance. Instead, they help you think clearly about the best time to take bpc 157 and tb 500 relative to your daily load and recovery.
Framework A: Post-training / post-activity alignment
Use this if your injury is irritated by training and you want dosing after you’ve finished the session.
- BPC-157: take after training or after the activity that typically aggravates the area.
- TB-500: take later in the day on the same training day (or on rest days) to support ongoing recovery without stacking stressors.
Why it works (logic): it reduces the chance you’re pairing the peptide effect window with peak mechanical stress.
Framework B: Sleep-window alignment
Use this if your routine is stable and your biggest recovery gains come from good sleep.
- BPC-157: take earlier in the evening so it’s well before bedtime.
- TB-500: take on days you’re trying to maximize rest—commonly evening dosing on non-training days.
Why it works (logic): it helps you standardize timing around the body’s natural repair/rest environment.
Framework C: Split dosing across a consistent daily rhythm
If your schedule allows two daily anchor points, split timing can reduce “all-at-once” variability.
- BPC-157: morning and early afternoon anchor (or morning and after work).
- TB-500: morning anchor on consistent days, with adjustments based on tolerability and perceived response.
Why it works (logic): it improves adherence and gives you clearer tracking of what you felt when.
Choosing the schedule: BPC-157-first vs TB-500-first thinking
Many people ask whether they should take BPC-157 or TB-500 first, or whether one “overrides” the other. In practice, timing helps you implement a staged plan rather than guessing.
When BPC-157-first scheduling tends to make sense
If your primary bottleneck is local pain, limited range of motion, or tendon/ligament irritation, I’ve seen people prioritize BPC-157 timing around symptom flares and training load. You can then add TB-500 later to support the broader recovery timeline.
When TB-500-first scheduling tends to make sense
If your main constraint is sustaining training while tissue heals (you need the schedule to “keep the machine moving”), some users place more emphasis on TB-500 timing on days with moderate activity, then use BPC-157 to target flare-ups.
Key takeaway: “best time” depends on which bottleneck you’re trying to solve first.
Safety and limitations: what to keep realistic
It’s important to keep your expectations grounded. Peptides discussed online are not universally standardized in quality, purity, or dosing guidance across sources. In my own workflow, I emphasize three practical guardrails:
- Quality control matters: inconsistent product quality can make timing seem ineffective.
- Track outcomes objectively: use pain scores, range-of-motion notes, and training volume logs so “timing worked” is measurable.
- Adjust based on tolerability: if you feel off, revise timing before continuing blindly.
If you’re dealing with a medical condition, taking other medications, or have an injury that could require diagnosis, involve a qualified clinician for individualized guidance.
FAQ
What is the best time to take bpc 157 and tb 500 if I train in the evenings?
A common approach is post-training alignment: take BPC-157 after your workout (when irritation is lowest), and place TB-500 later in the day or on rest days to support recovery without pairing it with peak mechanical load.
Should I take BPC-157 and TB-500 at the same time?
They don’t need to be simultaneous for timing to be effective. Many people choose separate timing anchors (morning vs evening, or post-training vs rest-day) so they can track response and adjust tolerability more clearly.
How long should I run a timing adjustment before deciding it doesn’t work?
In practice, I treat timing changes like a short experiment: keep the schedule consistent for a defined window (often 1–2 weeks) while tracking pain, function, and training tolerance. If your metrics don’t move and tolerability is stable, consider revising timing around your most consistent recovery anchor (sleep or post-training).
Conclusion: a practical next step
BPC-157 vs TB-500 isn’t just a choice of peptide—it’s a schedule design problem. The best time to take bpc 157 and tb 500 is the time that best matches your training load, sleep window, and symptom pattern while remaining consistent enough for you to measure results.
Next step: for your next 7–14 days, pick one timing framework (post-training or sleep-window), keep the dosing anchors consistent, and log pain score + range of motion + what activities were tolerated. Then adjust timing based on your observed response—not just internet recommendations.
Discussion