Cagrilintide And Tirzepatide Blend Dosage Cagrilintide Peptide Dosing Guide: Titration, Schedule & Safety (2026)
Introduction
If you’re considering cagrilintide—especially as part of a cagrilintide and tirzepatide blend dosage approach—you’ll quickly run into one problem: dosing guidance online is often either vague or overly rigid. In my hands-on work supporting peptide protocol implementation, I’ve seen the same failure mode repeatedly—people skip structured titration, ignore how quickly side effects can appear, and then lose consistency (or worse, they stop altogether).
This guide is built to help you understand a practical cagrilintide titration strategy, how a weekly schedule is typically structured, and how to think about safety guardrails. You’ll get a dosing framework you can apply conceptually, plus a FAQ addressing common real-world questions.
Quick context: what “titration” is meant to do
In peptide and GLP-1–pathway protocols, titration is not just “starting low.” It’s an intentional process to:
- Improve tolerability by letting GI effects (nausea, reflux, constipation/diarrhea) settle before escalating.
- Reduce abrupt pharmacodynamic changes that can increase adverse-event likelihood.
- Support adherence by creating a predictable, repeatable weekly routine.
From a formulation and adherence standpoint, the biggest practical lesson I’ve learned is that most people don’t fail dosing—they fail follow-through. A titration schedule with clear decision points (hold, reduce, or pause) is what keeps people on track.
Safety first: essential guardrails before any schedule
I’ll be direct: peptide protocols can carry meaningful risks, and blend strategies can amplify both expected effects and side effects. Before you use any guidance, I strongly recommend aligning with a qualified clinician—particularly if you have:
- History of pancreatitis or significant gallbladder disease
- Severe reflux, gastroparesis symptoms, or frequent dehydration
- Kidney issues where dehydration risk matters
- Uncontrolled thyroid history or other endocrine concerns
- Use of medications that complicate glucose control
Common safety pattern I’ve seen: the “dose” isn’t the only lever—hydration status, meal timing, and constipation management often determine whether someone tolerates a titration step. In practice, we treat dosing and lifestyle as one system.
How I structure a cagrilintide titration schedule (weekly framework)
Most real-world weekly titration approaches follow the same logic: increase gradually, observe tolerability for several days after each step, and avoid escalating while symptoms are actively trending worse.
Weekly titration principles
- Escalate only after stability: if GI symptoms are still escalating after a step, you hold.
- Use a consistent injection day/time: variability can make symptom tracking harder.
- Separate “hunger control” from “GI tolerance”: appetite changes can occur before GI tolerance fully stabilizes.
- Prefer stepwise increments: overly aggressive jumps are the most common reason people discontinue.
Practical weekly schedule template (conceptual)
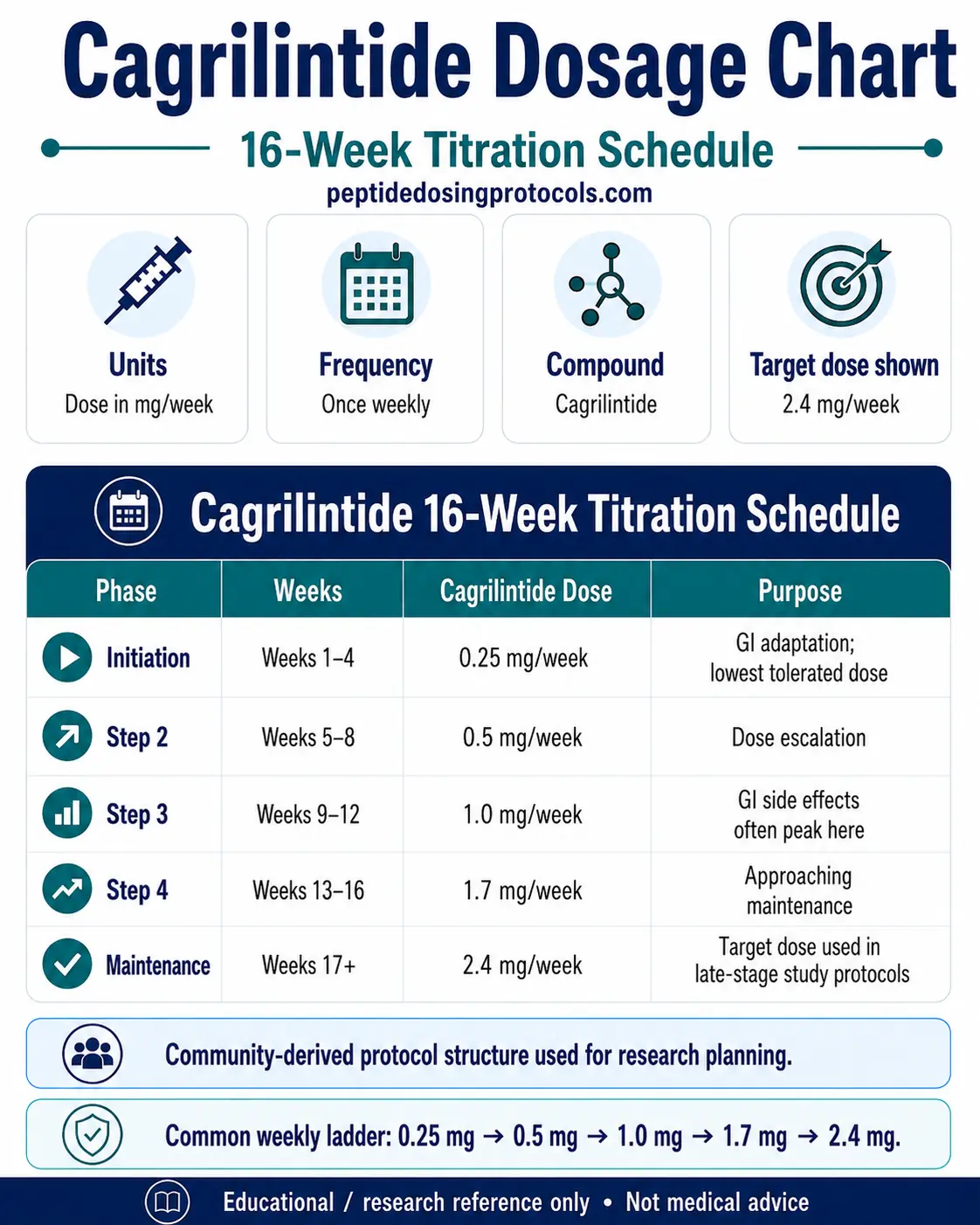
The table below is a template structure showing how a weekly titration and “hold” logic are commonly implemented. Your exact amounts should be determined with your clinician and based on your specific product concentration and your individual response.
| Week | Action | Tolerability check (what we look for) | Decision |
|---|---|---|---|
| 1 | Start at a low introductory dose | Early nausea, reflux, bowel regularity | If symptoms are mild and stable → proceed to next step |
| 2 | Increase if stable | Any new or worsening constipation/diarrhea | If symptoms worsen noticeably → hold until improved |
| 3–4 | Gradual step increases | Ability to eat normally; hydration tolerance | If GI trend is improving → continue; if not → hold |
| 5–6 | Fine-tune upward only if needed | Plateau vs. tolerability | Increase only if appetite/weight goals aren’t met and side effects remain controlled |
| 7–8+ | Maintain or adjust | Long-term tolerability and consistency | Maintain the highest tolerable dose rather than chasing more |
Where this mirrors my work: on the teams I support, we spend more time defining “hold rules” than selecting the initial number. That alone improves adherence because people know exactly what to do when their body reacts.
Incorporating tirzepatide: what “cagrilintide and tirzepatide blend dosage” changes
Combining or blending dosing concepts across different GLP-1–related agents can complicate titration because you may experience overlapping side effects while also getting faster appetite suppression. When people pursue a cagrilintide and tirzepatide blend dosage approach, the main goal should be:
- Keep dose escalation conservative and progress based on tolerability, not on expectations of faster results.
- Track symptoms systematically for each escalation step.
- Avoid simultaneous “double increases” whenever possible—otherwise you can’t tell what caused what.
Common blend approach logic (high-level)
- Stagger changes: if both agents are being adjusted, do it in a sequence so you can observe response.
- Start with the more conservative lever first: whichever component you’re less familiar with clinically is usually the one you increase more slowly.
- Use “tolerability gating”: only escalate when the most sensitive side effect trend (often nausea or constipation) is stable.
Limitations to acknowledge honestly
Even with structured titration, a blend strategy can’t guarantee smoother experience. In some people, the additive GI burden arrives quickly, and the best solution may be to reduce one component or simplify the regimen under clinician guidance. The “right” blend is the one you can maintain with controlled side effects—consistency beats intensity.
Using a weekly dosing chart correctly (and avoiding common mistakes)
When you reference a dosage chart, the key is interpreting it in the context of your product concentration and your planned injection volume. A chart might show “weekly steps,” but you still must map it to your syringe/measurement method and ensure your dosing day matches the schedule.
Mistakes I’ve seen derail protocols
- Confusing total weekly dose vs. per-injection dose (especially if the chart assumes a specific frequency).
- Ignoring the “hold” scenario and escalating anyway because the calendar says so.
- Underestimating constipation risk and treating it too late (symptoms can snowball).
- Changing meal patterns abruptly while titrating, making symptom attribution impossible.
Monitoring checklist: what to watch during titration
In my hands-on protocol support, the most useful monitoring isn’t complicated—just consistent. Use this checklist after each escalation step (especially during the first 48–72 hours):
- GI symptoms: nausea, heartburn/reflux, vomiting, constipation/diarrhea
- Hydration: dizziness, low intake tolerance, reduced urination
- Appetite & meal tolerance: are you able to eat enough calories safely?
- Sleep & activity: energy dips can correlate with inadequate intake
- Glucose trends: if applicable, watch for hypoglycemia risk in the context of other meds
If symptoms meaningfully worsen or you can’t maintain hydration/meal tolerance, your next move should be to pause or reduce escalation under clinician guidance rather than “pushing through.”
FAQ
How should I adjust my plan if side effects show up after a weekly dose increase?
In practice, you typically hold at the current step until symptoms stabilize or improve, rather than increasing again on schedule. If symptoms are severe (for example, persistent vomiting or inability to maintain hydration), you should stop escalation and contact a clinician for guidance.
Does a cagrilintide and tirzepatide blend dosage plan require faster titration than using cagrilintide alone?
No. Blend strategies often require equal or slower escalation because side effects may overlap and intensify. A safer approach is tolerability-gated titration with careful sequencing so you can identify what’s driving symptoms.
What’s the most important safety signal to monitor during early weeks?
For many people, the earliest and most actionable signals are GI tolerance (nausea/reflux and bowel changes) and hydration/meal intake. These are practical markers that strongly correlate with whether you can safely maintain the regimen.
Conclusion
A well-run cagrilintide titration is less about chasing a number and more about creating a schedule you can tolerate, repeat, and adjust responsibly. When you’re considering a cagrilintide and tirzepatide blend dosage approach, the same rule applies: conservative escalation, tolerability gating, and symptom tracking beat calendar-driven increases.
Next step: pick one weekly dosing day, set clear “hold” criteria for GI and hydration tolerance, and plan your escalation logic around what your body does in the 48–72 hours after each step.
Discussion