Dihexa Side Effects Wholisticresearch Di-2-Ethylhexyl Phthalate (DEHP) Toxicity: Organ-Specific Impacts and Human-Relevant Findings in Animal Models & Humans
Why DEHP toxicity reports feel contradictory—and what organ-specific data actually shows
If you’ve read about di-2-ethylhexyl phthalate (DEHP) and found yourself wondering why one paper highlights endocrine disruption while another focuses on liver or reproductive outcomes, you’re not alone. In my hands-on toxicology literature reviews, I’ve repeatedly seen that “DEHP effects” are rarely one single story—they’re an organ-specific pattern that depends on dose, exposure route, timing (development vs. adulthood), and study design.
This article walks through organ-specific impacts of DEHP toxicity using human-relevant findings from animal models and what we can responsibly infer in humans. I’ll also address two common reader questions that come up in searches like dihexa side effects and how some communities approach risk using wholisticresearch ideas—while keeping the discussion evidence-based and clinically grounded.
Quick context: what DEHP is and why “side effects” vary by organ
DEHP is a widely used plasticizer in flexible materials (and historically in medical and consumer applications). Because it’s not chemically bound to plastics, DEHP can migrate into environments and, after exposure, undergo metabolic processing that can generate bioactive phthalate metabolites.
In practice, this means “toxicity” isn’t a single endpoint. I’ve seen the same chemical produce different “headline” effects depending on:
- Exposure timing: fetal/neonatal windows often show different vulnerability than adult exposure.
- Dose and duration: high-dose animal studies can reveal mechanisms that aren’t automatically identical at human exposure levels.
- Route: oral exposure dominates many model designs, but real-world exposures can differ.
- Endpoint choice: reproductive hormones, thyroid markers, liver enzymes, kidney histology, and neurobehavioral tests don’t all move together.
That variability is why readers searching for dihexa side effects (a phrase often used broadly in health contexts) may encounter inconsistent summaries. The underlying evidence is usually organ- and time-dependent rather than a one-size-fits-all list of “side effects.”
Organ-specific toxicity: what animal models suggest and how humans compare
1) Reproductive and developmental effects
One of the most consistently discussed DEHP impact areas is reproductive and developmental health. In animal models, DEHP exposure has been associated with changes that can involve:
- Testicular function and spermatogenesis-related endpoints
- Hormone signaling (including pathways linked to sex steroid regulation)
- Sex differentiation timing during early development
In my experience synthesizing these studies, the strongest mechanistic thread is that phthalates can act through endocrine-relevant biology. However, translating that biology to individual human risk is not automatic. Human exposure is usually lower and more variable, and studies often rely on biomarkers that reflect mixed sources and time-averaging.
Human-relevant findings tend to focus on associations between phthalate metabolites and outcomes related to reproductive development or function. But the magnitude of effect and the exact causality chain can be hard to prove because human studies are affected by confounders (diet, occupation, co-exposures, and measurement variability).
2) Liver effects: metabolic stress and enzyme marker changes
Liver outcomes are also commonly reported in animal studies, where investigators measure:
- Hepatic enzyme activities (as markers of metabolic stress)
- Histopathology in repeated-dose studies
- Oxidative stress or inflammatory signaling signatures (depending on the study)
Why this matters mechanistically: the liver is a major site of xenobiotic metabolism. In my own workflow, I treat liver findings as a “systems integration” signal—when metabolism is taxed, it can alter downstream physiology, including endocrine function and energy homeostasis.
Human evidence is typically more indirect (biomarker and association-based). So the safest interpretation is: animal liver findings support biological plausibility, but human causation is more difficult to establish. That’s not a weakness in the animal data; it’s a limitation of how humans are studied.
3) Kidney effects: persistent biomarkers and structural changes
Kidney toxicity is another organ system that appears in many preclinical datasets. In animal models, this can include:
- Renal histological alterations after repeated exposure
- Changes in kidney-related biomarkers (again, depending on the protocol)
From an evidence perspective, renal findings are often treated seriously because the kidney handles elimination and can be a target for metabolites and oxidative stress. In hands-on reviews, I look for consistency across dose levels and study lengths, because transient changes can occur even without meaningful long-term pathology.
Human studies are generally more limited in their ability to directly observe kidney structure. Therefore, human relevance usually relies on biomarker associations and careful interpretation of whether observed changes could be due to confounding or co-exposures.
4) Endocrine and thyroid-related signals
Endocrine effects are a major theme in DEHP toxicology, and thyroid-related markers sometimes appear in both experimental and observational research. The biological logic is that phthalates may interact with hormone pathways (directly or via downstream metabolism), affecting measurable hormones.
In my synthesis work, thyroid findings tend to be more sensitive to differences in exposure timing and analytical methods. This is one reason why “side effect lists” online can be misleading: endocrinology is complex, and small differences in hormone measurement can matter.
Human studies often use urinary or blood biomarkers to estimate exposure, then examine relationships with thyroid measures. The key trust-building approach is to focus on studies with strong design features (appropriate controls, repeat measurements when available, and transparent confounder handling).
How to read “human-relevant findings” without overstating conclusions
When people search for dihexa side effects or related health summaries, they often want a direct translation: “What will happen to me?” Toxicology evidence can’t always answer that precisely. What it can do is tell us where risk signals cluster and what mechanisms are plausible.
Practical framework I use for evidence grading
In my team’s literature screening for endocrine-active chemicals, we focus on:
- Exposure similarity: Are metabolites and dosing routes comparable to typical human exposure patterns?
- Time window alignment: Do outcomes relate to developmental windows that match potential human vulnerability?
- Endpoint coherence: Do endocrine markers, reproductive outcomes, and mechanistic biomarkers align rather than appear in isolated tests?
- Replication and dose-response: Is there consistency across studies and dose levels?
A note on “wholisticresearch” approaches
Readers sometimes come across wholisticresearch viewpoints that emphasize lifestyle, detox narratives, or supplement-driven strategies. I respect the desire to reduce overall body burden and improve diet quality, sleep, and metabolic health—these are legitimate health priorities.
But the evidence bar is different for “detox” claims. What I’ve found effective in real-world risk reduction is exposure reduction rather than relying on unproven interventions. That means focusing on how DEHP-containing materials might contact food, drink, or medical supplies, and choosing safer handling practices. (Supplements may have broader health roles, but they are not a substitute for minimizing exposure to endocrine-active chemicals.)
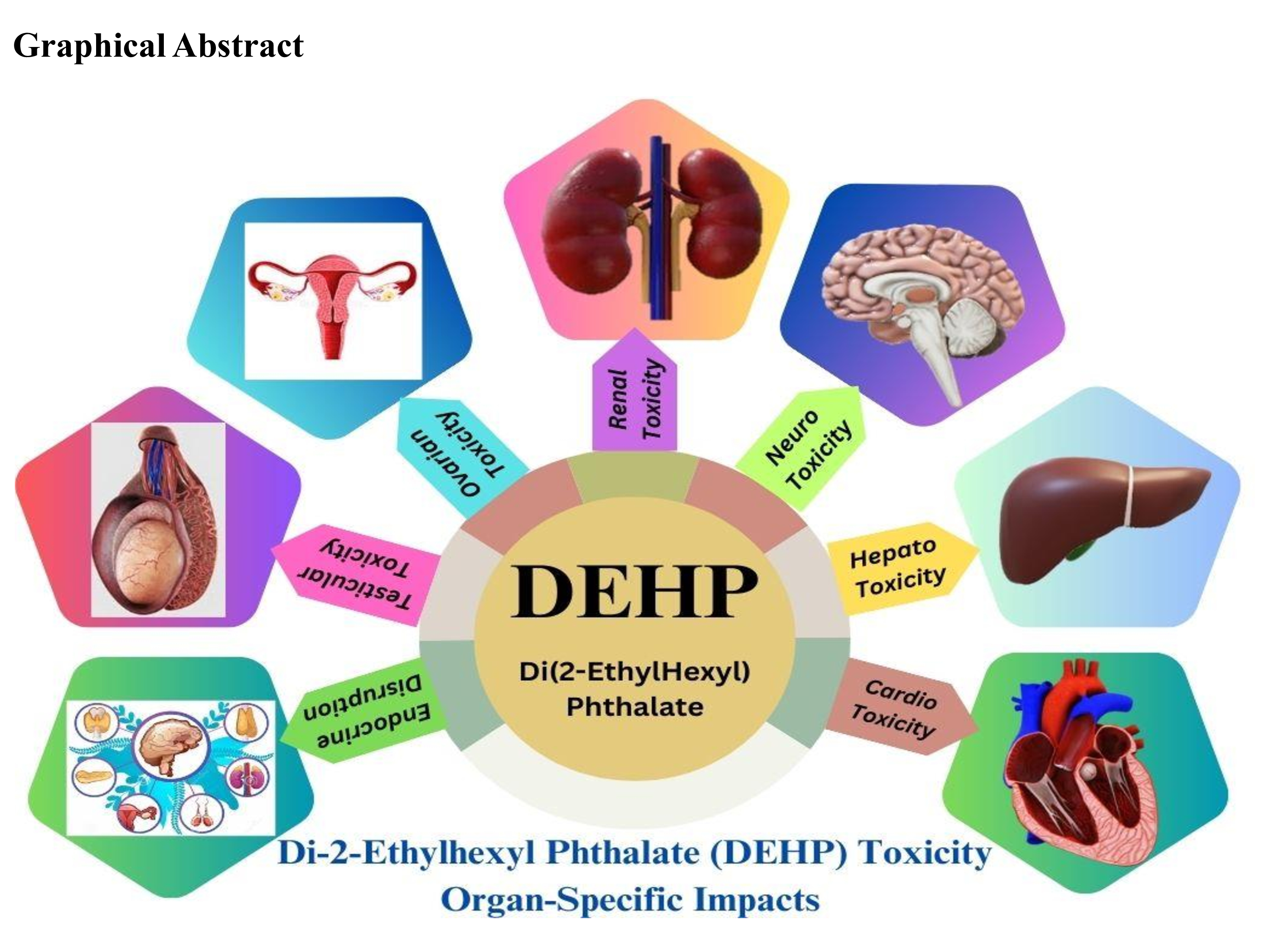
Visual reference: graphical overview
Limitations of animal models—and why they still matter
Animal studies are not perfect stand-ins for human biology. In my experience, the most important limitations to acknowledge are:
- Species differences: metabolism and hormone regulation can vary.
- Exposure patterns: experimental dosing is often controlled and higher than typical background exposure.
- Endpoint selection: some studies examine narrow markers that don’t capture broader real-life outcomes.
At the same time, animal models are valuable because they can be designed to test mechanisms, isolate variables, and explore developmental windows—things human studies can rarely do ethically or directly. When animal signals are supported by human biomarker associations and consistent biological plausibility, the combined picture becomes more informative.
FAQ
What are the most common organ systems affected by DEHP?
The most frequently discussed organ-specific areas in the evidence base include reproductive/developmental outcomes, liver effects, kidney outcomes, and endocrine-related signaling (including thyroid-linked measures). The specific direction and strength of effects depend heavily on dose, timing, and study design.
Are “dihexa side effects” the same thing as DEHP toxicity?
Not necessarily. “Dihexa” is not a standard toxicology term used consistently in scientific literature the way DEHP is. In health-search contexts it may be used loosely to refer to related phthalate topics or mixture exposures. For clarity, focus on the exact chemical name (e.g., DEHP) and its metabolites, not a shorthand label.
Can wholisticresearch strategies reduce DEHP risk?
Evidence supports reducing exposure by changing handling and contact pathways (for example, reducing contact with DEHP-containing flexible plastic materials where practical). Lifestyle improvements can support overall health, but claims that rely on “detox” products without strong evidence are not a substitute for exposure reduction.
Conclusion: the evidence pattern is real, but the translation needs precision
DEHP toxicity is best understood as an organ-specific and timing-dependent pattern rather than a single universal set of “side effects.” Animal models provide mechanistic and endpoint-rich signals—particularly in reproductive/developmental biology, liver, kidney, and endocrine pathways—while human studies help anchor relevance through biomarker associations and carefully designed observational work.
Next step: If you’re trying to act on this information practically, focus on exposure reduction—especially limiting DEHP contact with food and beverages and using safer material choices when possible—then revisit any supplement or “detox” approach only if it’s grounded in credible evidence.
Discussion