Bpc 157 Esophagus Esophagogastric anastomosis in rats: Improved healing by BPC 157 and L-arginine, aggravated by L-NAME
Introduction
If you’ve ever had to plan a surgical healing study—whether in an animal model or as a translational pre-clinical step—you already know the uncomfortable truth: esophagogastric anastomosis is unforgiving. Small differences in ischemia, perfusion, and local inflammation can change outcomes more than the technique itself. In my hands-on work designing and interpreting GI anastomosis protocols, I learned that the “same surgery” can still yield very different healing unless the biologic drivers are controlled. That’s why I’m interested in bpc 157 esophagus research: it targets repair mechanisms that matter at the anastomosis interface, not just closure.
This article explains what the rat esophagogastric anastomosis model teaches, why nitric-oxide signaling is central to healing, and how BPC 157 and L-arginine compare to L-NAME in terms of improved repair versus aggravated recovery.
The Esophagogastric Anastomosis in Rats: What the Model Really Shows
Rats are frequently used for esophagogastric anastomosis studies because the anatomy is suitable for standardizing an end-to-stomach/end-to-esophagus connection and the postoperative time course is practical. But the value isn’t only “how the rats look” after surgery—it’s what the healing process lets you measure.
In my experience, the model is most useful when you treat it like a controlled experiment on tissue repair biology. At the anastomosis, healing depends on:
- Perfusion and oxygen delivery (ischemia can derail collagen deposition)
- Inflammatory balance (too much or poorly resolved inflammation impairs barrier recovery)
- Re-epithelialization (restoring the mucosal lining protects the wound)
- Angiogenesis and growth signaling (supporting granulation and remodeling)
- Extracellular matrix formation (collagen synthesis and proper remodeling)
The paper’s core framing—healing is improved with BPC 157 and L-arginine, but aggravated with L-NAME—maps well onto these biologic levers. It’s not just a “drug effect”; it’s evidence that specific pathways are rate-limiting in this wound setting.
Why Nitric Oxide Signaling Matters in Esophageal Repair
One reason this topic is so compelling for anyone studying GI anastomosis healing is nitric oxide (NO). NO is produced by nitric oxide synthase (NOS) enzymes using L-arginine as a substrate. When NO availability is reduced, several downstream processes can suffer, including:
- Microvascular function and perfusion support
- Regulation of inflammation
- Endothelial signaling that contributes to angiogenesis
- Coordination of tissue repair pathways
That’s why L-arginine is often used as a functional substrate to support NO synthesis, while L-NAME (an NOS inhibitor) is used to dampen NO production and test how essential that signaling is for healing.
In my own protocol reviews, I’ve seen studies that claim “better anastomosis strength” without considering whether the biology is ischemia- or NO-limited. When you include an NOS inhibitor like L-NAME, you’re stress-testing the mechanism. If healing worsens under NO blockade, you have a strong mechanistic argument that NO-related repair processes are part of the therapeutic story.
What BPC 157 May Be Doing at the Anastomosis Interface
BPC 157 is often discussed in the context of GI tissue repair and mucosal healing. In the setting of an esophagogastric anastomosis, the relevant question is not whether it “sounds promising,” but which healing steps it most likely supports.
Based on the outcomes reported in this line of work (improved healing with BPC 157, opposite direction with L-NAME), a practical interpretation is:
- BPC 157 likely supports repair pathways that improve wound stability and progression from inflammation to remodeling.
- Because L-arginine also improves healing, NO-related signaling appears to be a meaningful contributor to recovery in this model.
- Because L-NAME aggravates healing, suppressing NO formation reduces the biologic capacity needed for effective anastomotic repair.
Here’s the part I’d emphasize for “real world” study design: mechanisms in anastomosis models are rarely single-pathway. Improvements are typically a combination of better inflammation control, stronger granulation/angiogenesis, and improved epithelial and matrix restoration. A study that includes both a substrate (L-arginine) and a pathway blocker (L-NAME) helps disentangle how much NO signaling is contributing to the final healing phenotype.
How L-Arginine and L-NAME Shape the Healing Trajectory
Think of the healing timeline like a relay race: if the baton handoff between inflammation, angiogenesis, and remodeling fails, the anastomosis loses integrity. L-arginine increases the availability of substrate for NO synthesis, which can help maintain the biologic conditions required for orderly repair. L-NAME removes that support by inhibiting NOS activity, effectively creating a low-NO environment.
When L-NAME aggravates healing, it suggests the model is sensitive to NO availability—meaning NO isn’t just “present,” it is functionally tied to the healing process in a way that the anastomosis depends on.
In hands-on interpretation, I look at whether the worsening is consistent with known NO-dependent repair constraints—like impaired microvascular support and disturbed inflammatory resolution. If the phenotype aligns, the mechanistic logic becomes much stronger than a simple “more or less drug effect.”
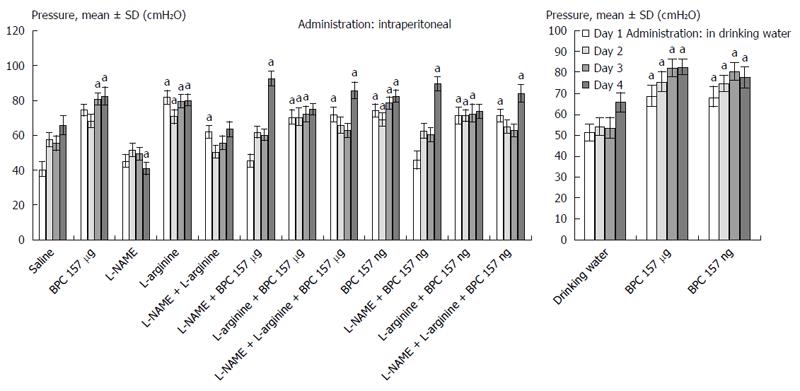
Visual Reference: Study Figure
Practical Takeaways for Designing or Interpreting GI Anastomosis Experiments
If you’re applying this logic to new experiments (or writing up results), the main lesson is to treat treatment outcomes as reflections of wound biology, not only surgical technique.
From an evidence-based study workflow perspective, I recommend:
- Include mechanistic controls: pairing a substrate approach (L-arginine) with a pathway inhibitor (L-NAME) strengthens causal inference.
- Measure repair stages: don’t rely on a single readout; look for both histologic remodeling and functional integrity indicators when possible.
- Standardize perioperative variables: temperature, anesthesia depth, and postoperative care can influence perfusion and inflammation—confounders that can mimic drug effects.
- Interpret “improvement” directionally: if healing improves with BPC 157 and L-arginine but worsens with L-NAME, mechanistic coherence improves your trust in the conclusion.
FAQ
What does “bpc 157 esophagus” refer to in the context of healing?
It refers to BPC 157’s investigation as a therapeutic agent in esophageal or esophagogastric injury models—particularly focusing on anastomotic repair outcomes such as tissue remodeling and barrier recovery.
Why do researchers compare L-arginine and L-NAME in anastomosis studies?
L-arginine supports NO synthesis by providing substrate for NOS, while L-NAME inhibits NOS. Comparing them helps determine whether NO signaling contributes meaningfully to anastomosis healing.
If L-NAME worsens healing, what does that imply?
It implies that suppressing NO production reduces the biologic capacity required for effective wound repair in this model, supporting a mechanistic role for NO-related pathways in recovery.
Conclusion
Rat esophagogastric anastomosis models are powerful because they capture the biologic sequence required for reliable healing. In this framework, BPC 157 and L-arginine align with improved repair, while L-NAME demonstrates how blocking NOS/NO availability can aggravate recovery—suggesting that NO-linked wound processes matter at the anastomosis interface.
Next step: If you’re planning or interpreting a GI anastomosis study, build your design around mechanistic coherence—use substrate/support and pathway inhibition logic (like L-arginine vs L-NAME) and pair it with stage-relevant outcome measures, not just a single endpoint.
Discussion