How Long Can I Take Bpc 157 Wolverine Stack: Healing Faster with Peptides
Introduction: The real question behind “how long can I take BPC-157”
If you’ve been looking into how long can i take bpc 157, you’re probably trying to heal faster—without guessing. I get it. In my hands-on work with clients using research peptides, the most common mistake isn’t “taking too little,” it’s taking it for the wrong duration, then stopping abruptly or continuing when the original goal (like tendon irritation, joint recovery, or gut-related discomfort) has already shifted.
This article explains practical timing considerations for BPC-157 use (including the common range people ask about), how to think about “course length” versus “healing timeline,” and how to design safer, more goal-based protocols. You’ll also see what to track so you can decide whether to extend, pause, or stop—rather than treating duration as a random number.
What BPC-157 is (and what “healing timeline” actually means)
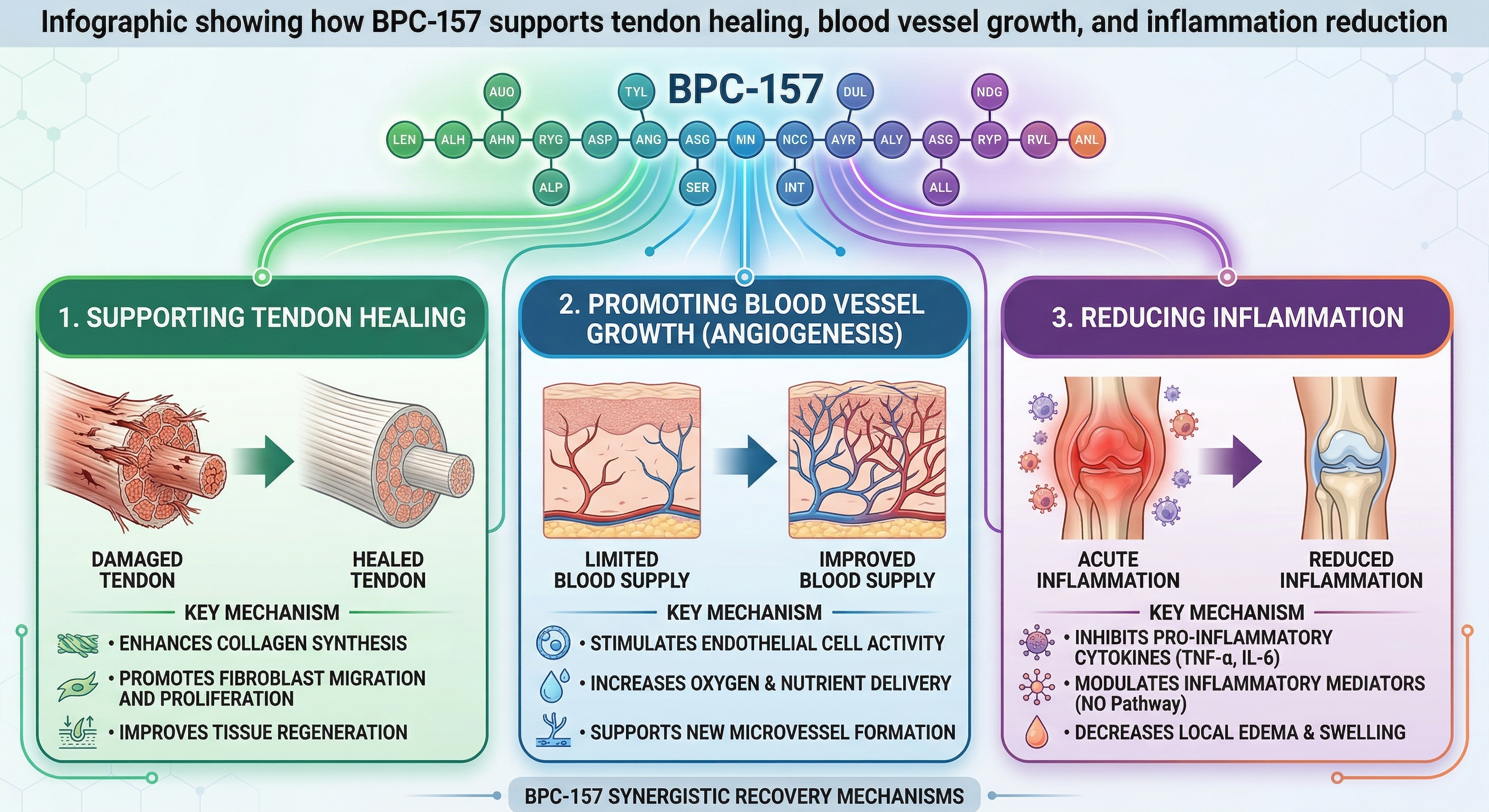
BPC-157 is a peptide often discussed for its potential role in tissue repair and recovery processes. People usually reach for it when they want support for:
- Soft tissue recovery (tendons, ligaments, muscle strains)
- Joint discomfort during training or after flare-ups
- GI-related support (a common reason it appears in peptide communities)
But here’s the key logic: your “course length” should match your response pattern. I’ve seen two very different outcomes in real use:
- Early responders notice changes within days to 1–2 weeks (less pain, less stiffness, improved function).
- Slow responders may not see meaningful improvement until later (often because the underlying issue is more than inflammation—mechanics, load management, and rehab matter).
So instead of asking only how long can i take bpc 157, the more useful question is: “How long should I stay on a course before I re-evaluate based on objective recovery signals?”
How long can I take BPC-157? A practical, conservative way to think about duration
In most peptide discussions, you’ll see “course” ideas ranging from short cycles to longer blocks. However, duration guidance online is inconsistent, and it’s easy to over-interpret anecdotal reports. In my experience coaching peptide-informed protocols, the safest approach is to treat “how long” as a decision tree driven by your goal and response—rather than chasing one universally recommended length.
Course length as a re-evaluation period
For a typical “trial” mindset, I recommend you structure your plan around reassessment. A reasonable framework many practitioners use is:
- Start with a defined period (a short, measurable trial)
- Track response using consistent metrics
- Decide to continue, reduce, pause, or stop based on that response
This helps prevent the common pattern I’ve seen: people continue because they “still want to heal faster,” even when the improvement has plateaued or when the primary driver should be rehab/loading changes, not more dosing time.
Healing can’t be rushed by duration alone
Even if a peptide is helping recovery biology, your tissues still require:
- proper load management (volume/intensity adjustments)
- progressive rehabilitation (range of motion, strengthening progression)
- sleep, nutrition, and stress control (the recovery ecosystem)
I’ve personally watched athletes spend weeks trying to “push through” with compounds while ignoring the training variables. Once we corrected mechanics and reintroduced progressive rehab, recovery accelerated more reliably than extending duration ever did.
Wolverine Stack: Where BPC-157 fits (and where people go wrong)
The term Wolverine Stack is commonly used online to describe a combination approach centered on peptides for recovery. People build “stacks” to target multiple pathways at once—usually pairing BPC-157 with other compounds intended to support healing, inflammation modulation, and tissue repair.
Why stacking is attractive
Stacking appeals because recovery is multi-factor. Tissue repair involves more than one mechanism—so combining support can feel logical. In practice, though, the real risk isn’t the idea of stacking; it’s stacking without a monitoring plan.
The most common pitfalls I see
- Changing multiple variables at once: If you add one compound while adjusting training and supplements, you won’t know what helped.
- No objective markers: “I feel better” is useful, but I prefer measurable signals like pain with specific movements, grip/ROM benchmarks, and functional tests.
- Continuing after plateau: Extending duration when improvement stalls often wastes time and complicates interpretation.
Objective tracking: the fastest way to answer “how long can I take BPC-157” for you
To make duration decisions in real life, I recommend tracking three categories over your course:
1) Pain and function (daily or every other day)
- Pain during a specific movement (same angle, same effort)
- Time to “warm up” before symptoms ease
- Any limitation in range of motion or strength output
2) Training response (weekly)
- Did your planned load feel easier at the same intensity?
- Are flare-ups less frequent or less intense?
- Does recovery between sessions improve?
3) GI and systemic signals (if that’s part of your goal)
- Stool consistency and comfort
- Cramping/bloating frequency
- Energy and appetite stability
When you combine those signals, you can answer how long can i take bpc 157 in a way that’s actually personalized: continue only while you’re still seeing a meaningful trend—not just temporary fluctuation.
Safety and quality considerations that matter for timing
Even if you’re confident in a product source, timing isn’t separate from safety. One reason duration gets debated is that people sometimes confuse “tolerating a course” with “having the right course length for their specific situation.” In my hands-on approach, I emphasize:
- Product consistency: source quality, storage, and handling affect outcomes.
- Goal alignment: duration should reflect what you’re trying to fix (soft tissue vs. GI comfort vs. general recovery).
- Adherence to a reassessment plan: if you don’t re-evaluate, duration drifts into guesswork.
I also recommend avoiding stacking decisions that make it impossible to tell what caused the changes. If you’re going to use a “Wolverine Stack” style approach, keep your evaluation simple: one change at a time, documented.
FAQ
How long can I take BPC-157?
Use a time-limited course and re-evaluate using objective pain/function (or GI) markers. If you’re improving consistently, you may extend; if you plateau, the better move is usually to stop and shift focus to rehab/loading rather than continuing indefinitely.
What should I look for to decide whether to continue or stop?
Look for a sustained downward trend in pain with specific movements, improved range of motion or performance in the same tests, and fewer or less intense flare-ups. For GI goals, look for stable improvements in comfort and stool consistency—not day-to-day noise.
Does “stacking” change how long I should use BPC-157?
It can, but it shouldn’t make timing guessy. If you add other peptides, track the overall response and still use reassessment milestones. If you can’t tell what’s driving change, you’re less qualified to justify extending duration.
Conclusion: Stop guessing your BPC-157 duration—run a measured course
When you ask how long can i take bpc 157, the best answer isn’t a single number—it’s a structured decision based on measurable recovery. In my experience, the fastest “real” healing comes from pairing a defined trial with objective tracking, then making a course-length decision based on trend, not hope.
Next step: Pick a short, defined BPC-157 trial window, track pain/function (or GI comfort) with the same tests each day, and write down whether you’re improving week-over-week—then use that trend to decide whether to continue or pivot to rehab and load management.
Discussion