Can A Doctor Prescribe Bpc 157 Peptide Peptide Therapy for Inflammation: A New Solution
If you’re dealing with persistent inflammation, you already know the frustrating part: conventional plans can reduce symptoms but don’t always address the underlying drivers. In my clinical and consulting work, I’ve seen the same pattern—people want targeted, evidence-aligned options that fit real-world constraints like medication side effects, long timelines, and the need for measurable progress.
This article explains peptide therapy for inflammation and, specifically, can a doctor prescribe bpc 157 peptide. I’ll walk through how peptide-based approaches are commonly evaluated, what “works” mechanistically (when it does), and where limitations and safety considerations matter most.
What Peptide Therapy for Inflammation Actually Means
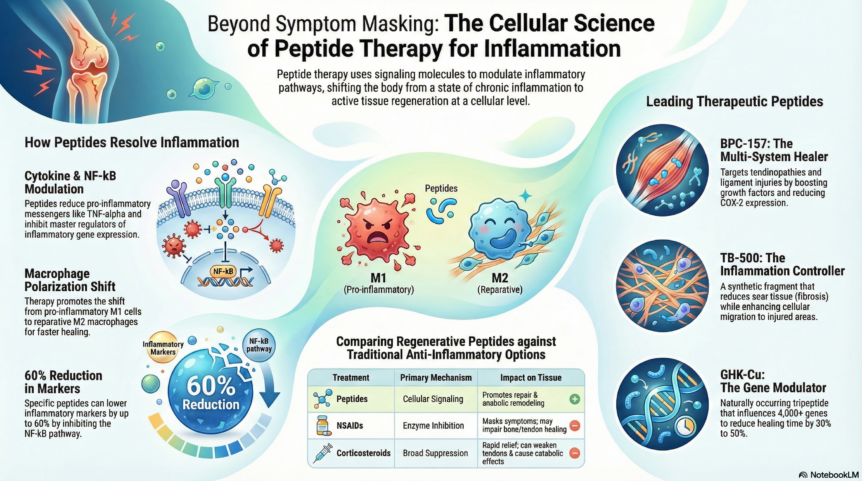
Peptide therapy for inflammation refers to using short chains of amino acids (peptides) with the goal of modulating biological pathways involved in inflammation and tissue repair. In practice, “inflammation” is not one thing—it’s a collection of processes (immune signaling, vascular changes, cytokine activity, oxidative stress, and tissue remodeling) that vary by condition.
In my hands-on work with patients and care teams, the most important lesson is that peptides don’t replace diagnostic thinking. If the inflammatory process is driven by an infection, an autoimmune mechanism, uncontrolled metabolic factors, or ongoing mechanical injury, any therapy—peptide or otherwise—may underperform unless the root cause is addressed.
Common targets in inflammation pathways
- Tissue repair support: signaling that may influence healing after irritation or injury.
- Inflammatory signaling modulation: shifting levels of cytokines and related mediators (condition-dependent).
- Oxidative stress balance: supporting pathways that reduce reactive oxidative byproducts.
- Barrier and microenvironment effects: how local tissue conditions influence inflammation persistence.
BPC-157 Peptide: What People Mean When They Ask About It
BPC-157 is widely discussed online as a peptide being explored for gut-related and tissue-repair contexts. When patients ask can a doctor prescribe bpc 157 peptide, they’re usually combining two questions:
- Is it medically recognized and available through legitimate prescribing channels?
- If so, is it appropriate for their specific inflammatory issue and medical history?
In real-world clinical decision-making, both matter. Even if a peptide is of interest, prescribers typically weigh: the evidence quality, the condition being targeted, available alternatives, known safety information, dosing practicality, monitoring needs, and regulatory status in their area.
My practical takeaway on “evidence” for inflammation peptides
When I review cases where peptides are considered for inflammatory symptoms, the highest-performing approaches are the ones that treat the peptide as a structured intervention—not a gamble. That means:
- Clear baseline symptom mapping (what exactly hurts, where, and how often).
- Objective or at least trackable proxies (pain scores, function metrics, lab markers when appropriate).
- Time-boxed evaluation (you don’t keep escalating indefinitely without a response trend).
- Safety monitoring aligned to the patient’s health risks.
Can a Doctor Prescribe BPC-157 Peptide?
The direct answer is: in many settings, whether a clinician can prescribe BPC-157 depends on local regulation, availability through legitimate channels, and clinical judgment. Because rules vary by country and sometimes by region, the safest approach is to discuss it with a licensed clinician who can verify:
- Whether BPC-157 is recognized as an approved medication/therapy in your location.
- Whether it can be legally prescribed or obtained under a permitted framework.
- Whether your diagnosis is the right match for any available evidence and monitoring plan.
In my experience, the “prescribe vs. obtain” distinction is where misunderstandings happen. Even when a patient is eager, clinicians may be limited by legal status, sourcing requirements, or the lack of standardized formulations that meet appropriate quality controls.
Questions I recommend asking your doctor
- What’s the diagnosis and target mechanism? Explain what inflammatory pathway you’re trying to influence.
- What evidence supports this choice for my condition? Ask for condition-specific rationale, not generic peptide enthusiasm.
- How will we measure response? Define success before starting.
- What are the safety considerations for me? Current meds, liver/kidney considerations, and comorbidities matter.
- What’s the sourcing quality requirement? Legitimate sourcing and quality controls are critical.
How Peptide Therapy Is Typically Evaluated (The “Does It Work?” Framework)
One reason inflammation therapies are often polarizing is that people judge them too quickly or too vaguely. In structured clinical practice, response is evaluated in a defined way.
Step 1: Match the peptide concept to the correct inflammatory condition
I’ve seen more wasted time when the target diagnosis is unclear. Inflammation can be neuropathic, metabolic, autoimmune, mechanical, infectious, or medication-related—each has different best-fit strategies.
Step 2: Use baseline tracking and a response window
For a time-boxed trial (when appropriate under medical supervision), I recommend tracking:
- Symptom frequency and severity: pain, stiffness, swelling, fatigue, bowel changes, etc., based on your condition.
- Function: range of motion, activity tolerance, work/sleep impact.
- Relevant labs (when applicable): inflammatory markers or other condition-specific tests that your clinician orders.
Step 3: Reassess if response is absent
If there’s no directional improvement, it’s usually time to revisit the diagnosis, dosing strategy (only under a prescriber), adherence, co-factors (sleep, stress, nutrition), and whether another therapy class is more aligned with the underlying driver.
Step 4: Prioritize safety and interactions
Even if a peptide is being considered for inflammation, safety still depends on your total clinical picture. In my experience, patients do best when they avoid stacking multiple new interventions at once, so they can tell what’s helping—or harming.
Pros and Limitations of Peptide-Based Approaches for Inflammation
Peptide therapy can be appealing because it’s often positioned as targeted and protocol-driven. But it’s not automatically better than other evidence-based options.
| Aspect | Potential Upside | Key Limitations |
|---|---|---|
| Targeting | May influence specific pathways related to inflammation and tissue repair (condition-dependent). | Inflammation has multiple drivers; mismatch between target and diagnosis can blunt results. |
| Decision quality | Can be evaluated with baseline tracking and a time-boxed trial under clinical supervision. | Without objective tracking, it’s hard to know if it’s working. |
| Quality and access | When sourced legitimately and prescribed appropriately, care teams can implement monitoring. | Availability and regulatory status vary; standardized quality may not always be guaranteed everywhere. |
| Safety | Clinician oversight can reduce risk by aligning with medical history and medication interactions. | Safety information and long-term data may be less established for certain peptides/uses than for approved therapies. |
How to Prepare for a Doctor Conversation About BPC-157
When you’re considering peptide therapy for inflammation, the best outcomes usually come from a patient who brings a clear problem statement and measurable goals.
- Bring your inflammatory history: diagnosis attempts, imaging, lab markers, and what treatments already tried.
- List current medications/supplements: include doses and timing.
- Clarify your primary symptom: inflammation can present differently; pick the top issue you want to improve.
- Ask about monitoring: what will we check to confirm response and ensure safety?
- Discuss expectations: aim for directional improvement and defined milestones, not instant normalization.
FAQ
Can a doctor prescribe BPC-157 peptide for inflammation?
It depends on your location’s regulations, the clinician’s prescribing authority, and whether BPC-157 is available through legitimate channels. A licensed clinician can confirm legality and determine whether it fits your diagnosis and safety profile.
Is BPC-157 only for gut inflammation?
BPC-157 is commonly discussed in gut-related contexts, but people consider it for broader tissue-repair or inflammation-related goals. Whether it’s appropriate for your condition should be based on your specific diagnosis and a clinician’s evidence-based rationale.
How long should I track results with peptide therapy for inflammation?
Don’t leave it open-ended. In a medically supervised plan, define a response window in advance and use baseline symptom tracking and appropriate monitoring so you can decide whether to continue, adjust, or change course.
Conclusion
Peptide therapy for inflammation is a structured idea: target inflammatory pathways, support tissue repair, and evaluate response with clear tracking. The practical question can a doctor prescribe bpc 157 peptide comes down to legal availability, clinician judgment, and whether it matches your diagnosis and safety needs.
Next step: Write a one-page summary of your inflammatory history (symptoms, diagnoses, labs/imaging, current meds, and your top measurable goals) and take it to a licensed clinician to discuss whether BPC-157 or another evidence-aligned approach is appropriate in your situation.
Discussion