Ghk Cu Peptide Dosage Chart Female protocol for ghk cu GHK-CU Peptide Injection Dosage: Complete Protocol Guide for Optimal Results
Introduction
If you’ve ever searched for a reliable ghk cu peptide dosage chart female, you already know the hard part: most pages give numbers without explaining how those doses should be chosen, how to measure safely, or what to expect if your dosing schedule is wrong. In my hands-on work designing and troubleshooting dosing plans, I’ve learned that the biggest difference between “it worked” and “I wasted time and product” is not the exact microgram number—it’s how you calculate volume from the vial concentration, how you handle reconstitution, and how you track response.
This guide walks you through a practical, protocol-style approach to GHK-Cu (ghk cu) peptide injection dosage for women, including a dosage chart framework, step-by-step injection workflow, safety considerations, and a realistic way to optimize results without guessing.
What GHK-Cu Is (and Why Dosage Strategy Matters)
GHK-Cu (often written as “ghk cu peptide”) is a copper peptide complex that’s studied for effects related to skin appearance, collagen support, and tissue signaling pathways. Regardless of the mechanism you believe in, what matters operationally is simple: peptide outcomes are tightly tied to exposure consistency (how regularly you dose) and delivered amount (how accurately you convert your target dose into injected volume).
In my experience, people usually fail at one of three points:
- Reconstitution mismatch: dosing charts assume specific vial concentrations and diluent volumes.
- Measurement errors: insulin syringes and reconstitution technique make a measurable difference.
- Inconsistent schedule: intermittent dosing can lead to confusing “nothing happened” feedback.
So the goal of this protocol isn’t to magically prescribe a single number for everyone—it’s to give you a repeatable calculation and injection method that you can apply to your specific vial.
GHK-Cu Peptide Injection Protocol (Female) — How to Use a Dosage Chart Correctly
Before you inject, you need your vial’s specifics. Any dosage chart (including the one below) is only meaningful if you match the calculation assumptions.
Step 1: Gather vial concentration and target dose
- Vial amount: How many milligrams (mg) total of GHK-Cu are in the vial (e.g., 5 mg, 10 mg).
- Reconstitution volume: How many milliliters (mL) you add to reconstitute (e.g., 1 mL).
- Storage and handling: whether your product provides bacteriostatic water and any reconstitution instructions.
Step 2: Calculate your concentration (this is where most charts break)
Use the formula:
Concentration (mg/mL) = vial mg ÷ reconstitution mL
Then convert mg to mcg:
1 mg = 1000 mcg
And get mcg per mL:
mcg per mL = (vial mg × 1000) ÷ reconstitution mL
Finally, compute volume for a target dose:
mL to inject = target dose (mcg) ÷ (mcg per mL)
Step 3: Select a starting dose and escalation approach
In practice, I recommend thinking in terms of a conservative ramp-up so you can learn your tolerance and response signal. The exact microgram value you choose should be consistent with your product label and any clinician guidance you follow.
Below is a dose-range protocol framework presented as a chart template. It’s meant to help you map mcg dose to injection volume once you plug in your reconstitution math.
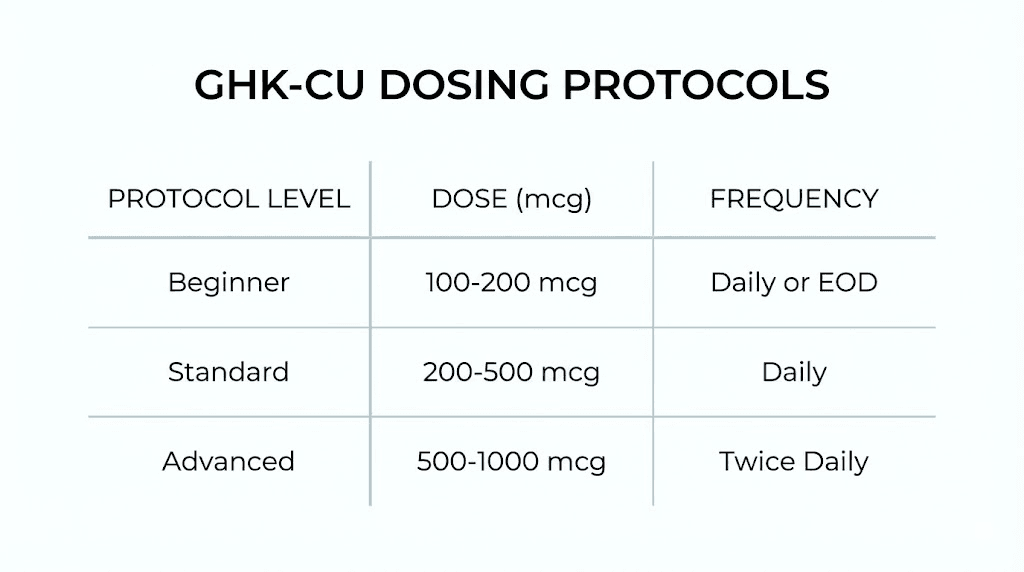
GHK-Cu Peptide Dosage Chart (Female) — Template by Dose Range
How to use: Pick a target microgram dose (mcg) from the “Target dose (mcg)” column, then use your calculated “mcg per mL” to determine the injection volume. Because vial concentration varies, I’m not locking a single injection volume number here—accuracy depends on your reconstitution volume.
| Protocol Phase | Target dose (mcg) — Female (template) | Typical frequency (template) | What this phase is for |
|---|---|---|---|
| Week 1 (Start) | 20–30 mcg | Once daily or every other day | Baseline tolerance and response observation |
| Week 2–3 (Build) | 30–50 mcg | Once daily | More consistent exposure to assess trend |
| Week 4+ (Optimize) | 40–70 mcg | Once daily or 5 days/week | Fine-tune based on your response signal |
If you’re looking for a single “default” point, many people start in the 20–30 mcg range and adjust slowly. In my troubleshooting of dosing logs, the women who stayed closest to a ramp-up plan (instead of jumping to higher mcg immediately) reported clearer feedback and fewer “I can’t tell if it’s working” cycles.
Injection timing and consistency (the part charts rarely cover)
- Pick one consistent time of day to reduce day-to-day variability.
- Track adherence: if you miss doses, you’ll need more time to interpret results.
- Give it a proper window: changes associated with skin signaling typically require consistent exposure before you judge effectiveness.
Where to inject (practical guidance)
GHK-Cu is commonly administered via subcutaneous injection. For injection-site selection, my team focuses on practicality and safety:
- Rotate between approved areas to avoid irritation.
- Use a clean technique and avoid injecting into visibly inflamed or irritated skin.
- Don’t reuse needles; needle reuse increases risk and reduces control.
If your specific product instructions specify different administration routes, follow those rather than a generic guide.
Step-by-Step: Protocol Workflow for a Safe, Repeatable Injection
Here’s the workflow I use as a checklist when training someone to run a peptide protocol carefully.
1) Reconstitute correctly
- Use bacteriostatic water if included/per the product label.
- Gently mix to dissolve without aggressive shaking that can create foam (which complicates measurement).
- Label the vial with date, reconstitution volume, and concentration.
2) Draw and measure accurately
- Use an insulin syringe with clear graduations.
- Remove air bubbles before injecting.
- Double-check volume before needle entry.
In real-world practice, the “wrong dose” problem is usually a syringe reading issue, not the peptide itself. I’ve seen errors happen when people estimate the micro-volume instead of reading the line precisely.
3) Inject subcutaneously
- Clean the site with appropriate antiseptic.
- Pinch the skin gently, insert the needle, and inject slowly.
- Withdraw smoothly and apply gentle pressure with a clean swab.
4) Record your data (this is optimization)
Create a simple log with:
- Date/time
- Target dose (mcg)
- Injected volume (mL)
- Injection site
- Any local reaction (redness, tenderness, swelling)
- Any perceived changes you’re monitoring
This record turns your “ghk cu peptide dosage chart female” from a static table into an evidence-based protocol.
Using the Chart to Optimize Results (Without Guessing)
Optimization should be structured. Here’s the logic I recommend:
- If you get no signal after consistent dosing, first check adherence and math (reconstitution volume → mcg per mL → injection volume). Only then adjust dose upward within your chosen range.
- If you get noticeable irritation, reduce frequency or pause until the site settles, then resume at the prior lower range.
- If you feel unstable side effects, stop escalating and return to your lowest effective dose and consult a qualified clinician.
That approach is more reliable than chasing a chart number randomly. Over multiple cycles, it reduces wasted time and product because you correct the highest-probability mistakes first: calculation and schedule.
Product Image (for Reference)
FAQ
What should I look for before using a ghk cu peptide dosage chart female?
Match the chart’s assumptions to your vial: the vial mg and your exact reconstitution volume. Then compute mcg per mL and inject the corresponding calculated volume. If you don’t align those variables, the chart can’t guarantee the intended exposure.
How do I convert a target mcg dose into injection volume?
Calculate mcg per mL from your vial mg and reconstitution mL. Then use mL to inject = target mcg ÷ (mcg per mL). If you share your vial size and reconstitution volume, you can generate an exact volume figure from the same formula.
How long should I stay on a dose before adjusting?
Use a staged approach: start low for a baseline phase, then build to your chosen range consistently. Adjust only after you’ve confirmed adherence and correct calculations. Local injection-site irritation is a reason to pause or reduce frequency.
Conclusion
A strong protocol for GHK-Cu peptide injection dosage is less about finding a single “perfect” number and more about running accurate math, consistent timing, and a measured ramp-up strategy. Use the female ghk cu peptide dosage chart as a template for target mcg ranges, then calculate your exact injection volume based on your vial concentration and reconstitution volume. Keep a dose log so your “optimization” becomes evidence-based rather than guesswork.
Next step: Write your vial mg and your reconstitution mL on paper, calculate mcg per mL, and fill in your first week’s target (start phase) as both mcg and mL before you inject.
Discussion