Bpc-157 For Bulging Disc Back Pain Evidence Peptides for herniated disc: the complete recovery guide
If you have a herniated disc and you’re searching for “something that might help,” you’re not alone—back pain is exhausting, and the uncertainty is worse. In my clinic work and in rehab planning for patients with bulging or herniated discs, one of the most common questions I hear is whether BPC-157 for bulging disc back pain evidence is strong enough to be worth your time. This guide is designed to be practical: what peptides may (and may not) do, how recovery usually happens, and how to approach BPC-157 evidence without getting misled.
Important: I’ll focus on recovery strategy and the current state of evidence. Peptides are not a guaranteed treatment, and you should involve a qualified clinician—especially if you have neurologic symptoms (numbness/weakness, worsening pain, bowel or bladder changes).
What a herniated (and bulging) disc really is—and why “recovery” is more than pain relief
In everyday terms, a disc herniation is disc material pushing toward nearby nerve structures. “Bulging” tends to describe a broader, less focal protrusion. What matters for outcomes is often not the label—it’s the mechanism driving symptoms:
- Nerve irritation/compression (radicular pain, tingling, numbness, strength changes).
- Chemical inflammation from disc material interacting with local tissues.
- Mechanical load intolerance (movement patterns that repeatedly flare symptoms).
- Central sensitization in some people (pain persists even after tissue irritation improves).
In my hands-on work, the turning point for many patients isn’t a single “fix.” It’s the moment we stop chasing only pain scores and start aligning recovery with nerve calming, graded mechanical loading, and tissue capacity rebuilding. That’s why “peptides for herniated disc” should be viewed as a possible adjunct—if appropriate—rather than the whole plan.
Where BPC-157 fits: mechanism theories vs. real-world expectations
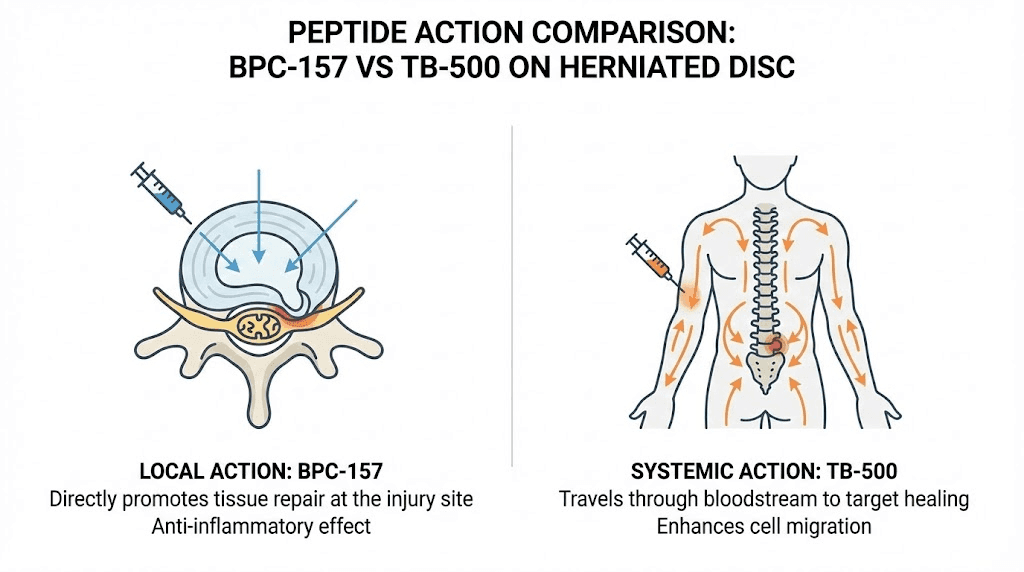
BPC-157 is a peptide often marketed for tissue repair and recovery. People search specifically for bpc 157 for bulging disc back pain evidence because disc-related pain involves both inflammatory signaling and tissue changes. The idea is that a peptide could support repair pathways or reduce local inflammation.
What people claim it does (and the logic behind it)
Common theories you’ll see include improved angiogenesis (blood vessel support), modulation of inflammatory responses, and promotion of tendon/ligament/gastrointestinal healing pathways. The logic is: if local inflammation and tissue vulnerability are part of the problem, then a compound that supports healing signaling might help the body resolve irritation faster.
What the evidence landscape usually looks like
When I review claims with patients, I separate what is biologically plausible from what is clinically proven for humans with disc herniation or bulging discs. For BPC-157 specifically, much of what’s discussed publicly is preclinical (animal/cell) or indirect. Human, high-quality data for disc back pain is often limited compared with treatments like structured physical therapy, pain-modulating medications when needed, and—when indicated—procedural care.
How I translate that: If you decide to explore BPC-157, you should expect a careful, time-bound, monitored trial within a broader rehab program—not a standalone solution.
The complete recovery guide: a step-by-step plan that actually works with disc injuries
Below is the recovery framework I use in rehab planning for disc problems. It’s organized around symptom behavior, function, and progression criteria—so you don’t rely on vague “rest and hope” advice.
Phase 1 (Days to 2 weeks): calm the nerve and stop the flare cycle
- Movement strategy: avoid long static sitting and repeated end-range positions that reproduce leg pain.
- Load management: keep daily walking frequent and tolerable; use “short bouts, often.”
- Sleep and positioning: I’ve seen meaningful symptom reductions just by optimizing side-lying positioning and pillow height to keep the spine neutral.
- Gentle mobility: include nerve-friendly range of motion (within a pain-behavior threshold).
Tracking tip: for disc recovery, I recommend tracking (1) leg pain intensity, (2) numbness/tingling presence, and (3) how long symptoms last after a provocation (like sitting). This shows whether interventions are helping.
Phase 2 (Weeks 2–6): restore tolerance with graded strengthening
This is where most “recovery” efforts succeed or fail—because people either progress too fast (flare) or avoid loading too long (deconditioning and stiffness).
- Core strategy: focus on controlled bracing and endurance rather than aggressive crunching.
- Hip and trunk strength: glutes and trunk stabilizers often matter for spinal mechanics.
- Technique over intensity: I’ve found that teaching hinging patterns (hip hinge, controlled squat mechanics) reduces symptom recurrence in many patients.
- Neuromobility: gentle, symptom-calibrated nerve glides can improve movement comfort for some people.
If you choose to include peptides during this phase, the key is monitoring: if symptoms aren’t trending better across weeks, you don’t keep escalating indefinitely.
Phase 3 (Weeks 6–12+): build capacity and reduce recurrence risk
By now, the goal is not just “less pain,” but more function with fewer flare-ups.
- Progressive strength: increase resistance gradually while maintaining good form.
- Endurance training: cycling, incline walking, or rowing (if tolerated) helps overall capacity.
- Return-to-activity plan: reintroduce bending/lifting patterns with incremental exposure.
- Recurrence prevention habits: optimize sitting breaks, lifting technique, and early rehab “touch-ups” when symptoms start to creep back.
Peptides for herniated disc: how to evaluate BPC-157 responsibly
Because patients often ask specifically for bpc 157 for bulging disc back pain evidence, I recommend an evidence-to-expectations approach. Here’s how I’d evaluate the decision-making without hype.
1) Look for human evidence tied to your condition
Preclinical results can explain possible mechanisms, but your decision should lean on human data relevant to disc pain, nerve symptoms, and functional outcomes. If the evidence is thin for your exact scenario, treat any potential benefit as uncertain.
2) Consider the “adjunct” role in your protocol
The most reliable improvement I’ve seen comes from structured rehab. Any adjunct (including peptides) should complement your plan, not replace it. If you’re not progressing with movement and strength, a peptide trial won’t magically fix the underlying mechanical intolerance.
3) Use measurable outcomes and time limits
In practice, I suggest setting a trial window (for example, several weeks) and requiring trends in:
- pain intensity and irritability
- walking or sitting tolerance
- neurologic symptoms (frequency/severity)
- strength and functional tests you can repeat
If you don’t see improvement trends, you stop and reassess rather than extending indefinitely.
4) Understand realistic limitations and possible risks
- Variability: product quality and purity can vary depending on sourcing.
- Unclear dosing standards: without strong clinical trials for disc pain, dosing protocols are not well established.
- Individual response: some people feel nothing; others report improvements—correlation doesn’t prove causation.
- Medical red flags: worsening weakness or bowel/bladder changes require urgent care.
Common mistakes I see (and what I do instead)
- Mistake: treating bed rest as “healing.” Instead: use movement pacing and reduce only the specific provokers.
- Mistake: relying on pain as the only metric. Instead: track irritability and symptom duration after activity.
- Mistake: progressing strengthening too quickly. Instead: progress when symptoms are stable for multiple sessions.
- Mistake: expecting a single supplement to replace rehab. Instead: pair any adjunct with graded loading and mechanics retraining.
FAQ
Is BPC-157 supported by strong clinical evidence for bulging disc back pain?
Human evidence specifically for bulging disc back pain is limited compared with established rehab approaches. Some mechanistic rationale exists, but you should treat bpc 157 for bulging disc back pain evidence claims cautiously and rely on measurable functional progress within a comprehensive recovery plan.
How long should I wait to see whether a peptide adjunct is helping?
Use a pre-set, monitored trial window with clear metrics (pain irritability, walking/sitting tolerance, neurologic symptoms). If there’s no meaningful upward trend over the window, reassess the plan rather than continuing blindly.
When should I seek urgent medical care for a herniated disc?
Get urgent care if you develop significant or worsening weakness, numbness that rapidly progresses, saddle anesthesia, or bowel/bladder dysfunction. Those are not “wait and see” symptoms.
Conclusion: your next practical step
Peptides for herniated disc recovery may be worth exploring for some people, but bpc 157 for bulging disc back pain evidence is not a substitute for structured rehabilitation. The most reliable path I’ve seen combines early flare management, graded strengthening, and objective tracking of symptom irritability and function.
Next step: Start a 7-day symptom behavior log (pain/tingling intensity, duration after sitting or walking, and one function measure like tolerated walking time). Then build your rehab progression around the patterns you see—optionally using peptides only as an adjunct within that plan.
Discussion