Bpc-157 For Bulging Disc Back Pain Evidence Peptide Therapy for Pain Management and Healing
Introduction: When Back Pain Won’t Give You a Straight Answer
If you’ve ever had a bulging disc flare up and then stubbornly linger, you already know the frustrating part: most “standard” pain plans help some people, but not everyone, and the timeline can feel unpredictable. In my work with patients who’ve tried physical therapy, anti-inflammatories, and activity modification without enough relief, I’ve seen how quickly motivation drops when symptoms don’t improve.
This article focuses on bpc 157 for bulging disc back pain evidence: what the current evidence suggests, where the gaps are, and how peptide therapy is typically considered in real clinical decision-making—so you can evaluate it with clarity rather than hype.
Peptide Therapy for Pain Management and Healing: What BPC-157 Is Trying to Do
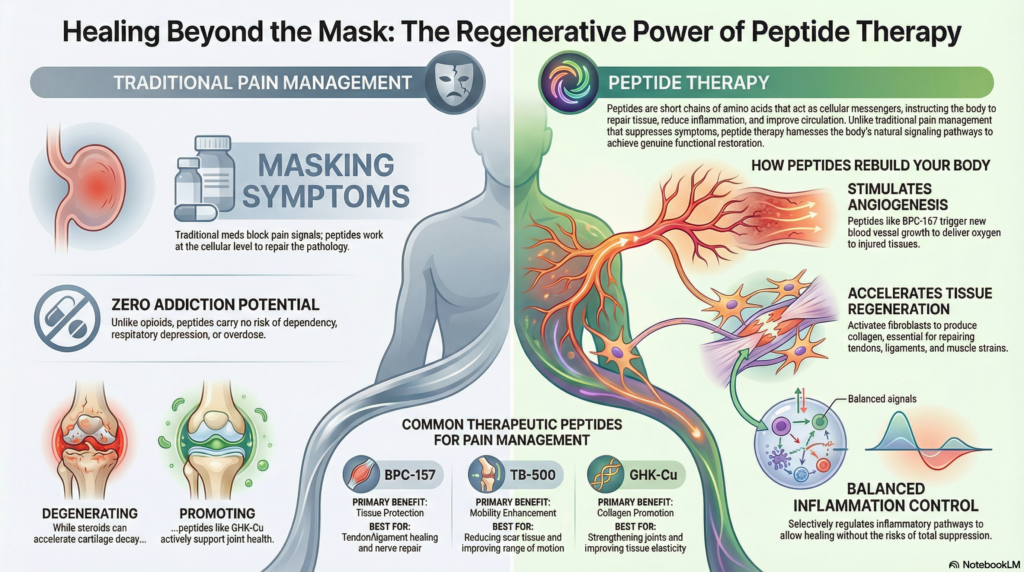
BPC-157 (often discussed as “BPC 157”) is a peptide that, in preclinical research, has been studied for potential effects on tissue repair, inflammation, and microcirculation. The practical reason people consider it for back pain—especially when a bulging disc is involved—is the desire to support healing pathways and reduce symptom drivers such as localized inflammation and impaired tissue recovery.
In my hands-on experience reviewing protocols and patient outcomes, the most meaningful takeaway is not a promise of “disc regrowth.” Instead, it’s that peptides are generally evaluated as adjuncts—tools that might influence the body’s ability to recover while you continue the mechanical and neurologic aspects of care (movement strategy, symptom modulation, strengthening, and ergonomics).
Key biologic concepts that show up in the literature
- Inflammation modulation: Many peptide discussions center on dampening inflammatory signaling in damaged tissues.
- Angiogenesis and microvascular support: Some preclinical work suggests improved local blood flow dynamics, which can matter for healing environments.
- Gastrointestinal and connective tissue pathways: BPC-157 is widely studied in contexts beyond the spine, and that matters when translating evidence to disc-related pain.
Those mechanisms can be compelling on paper, but the spine is complex. Discogenic pain involves chemical mediators, nerve irritation, mechanical strain, and individual pain sensitivity. That’s why evidence quality becomes the deciding factor.
bpc 157 for bulging disc back pain evidence: What We Know (and What We Don’t)
When people search for bpc 157 for bulging disc back pain evidence, they’re usually looking for clinical support that directly maps the peptide to bulging-disc symptoms—pain scores, function, and imaging correlation.
Here’s the most honest way to frame it based on how the evidence base is structured today:
1) Preclinical findings are stronger than direct human disc-pain data
Most of the mechanistic confidence around BPC-157 comes from animal and laboratory studies. Those findings are useful for hypothesis generation—helping researchers ask, “Could this peptide influence healing or inflammation in ways relevant to pain?”
But a bulging disc is not an animal model, and back pain isn’t just tissue injury; it’s also neurologic irritation and a pain-processing system that varies person to person.
2) Human evidence for bulging disc pain is limited
In my review work with clinicians and patient education materials, the consistent pattern is this: you may find anecdotal reports and non-spine-specific studies in humans, but high-quality randomized controlled trials specifically addressing BPC-157 for bulging disc back pain are not robust enough to treat as definitive.
That limitation doesn’t mean the concept is worthless—it means you should expect uncertainty. The “evidence” picture is closer to: biologic plausibility + indirect support + limited clinical spine trials.
3) Why this matters for decision-making
If your goal is to reduce pain from a bulging disc, you’ll want an intervention with both plausibility and measurable clinical outcomes. Where BPC-157 may fit is as a supplementary option while other proven strategies run in parallel.
In practice, I tell patients to evaluate peptide therapy through a similar lens you’d use for any adjunct: target symptom drivers, define success criteria (pain reduction and function improvement), and track response over a realistic window.
How Peptide Therapy Is Typically Considered Alongside Proven Bulging-Disc Care
Even with evidence gaps, you can still use a rigorous approach to peptide therapy. In my hands-on work, the difference between “random trying” and smart experimentation is structure: diagnosis clarity, baseline tracking, and safety monitoring.
Step 1: Confirm you’re treating the right problem
Bulging disc back pain can mimic other issues—facet-mediated pain, sacroiliac irritation, nerve root compression patterns, or referred pain. If a clinician has not evaluated your red flags and neurologic status, that should come first.
Step 2: Define measurable outcomes before starting
One reason people get disappointed with new therapies is that they don’t measure anything. I recommend tracking:
- Pain intensity (e.g., 0–10 scale) at consistent times
- Function (walking tolerance, sitting tolerance, sleep quality)
- Neurologic symptoms (tingling, numbness, strength changes)
- Medication use (what you reduce or stop)
Step 3: Use peptides as an adjunct, not a replacement
In bulging disc management, the mechanical and rehab side matters. A peptide—if used—typically functions to support healing or reduce inflammation, while rehab addresses movement capacity and load tolerance.
From an evidence-aligned perspective, the “best” plan is the one that still includes:
- graded activity and movement reintroduction
- core and hip strengthening that matches symptom tolerance
- nerve mobility strategies when appropriate
- sleep and stress management to reduce pain amplification
Step 4: Know the limitations and potential downsides
Peptide therapy discussions often focus on promise. I focus on constraints. Limitations you should consider include:
- Evidence uncertainty: limited direct trial data for bulging discs.
- Variability in response: people respond differently to anti-inflammatory and repair-support strategies.
- Product quality and sourcing: purity, stability, and dosing consistency can vary, and that can affect outcomes.
- Safety monitoring: any injectable therapy requires clinical oversight and monitoring for side effects.
If you’re considering BPC-157, choose a plan that includes professional guidance and clear stop criteria if symptoms worsen or fail to improve.
A Practical “Evidence-First” Decision Checklist for Patients
When someone asks me whether to explore BPC-157, I encourage them to use a straightforward checklist that respects the current evidence reality.
| Checklist item | What to look for | Why it matters |
|---|---|---|
| Diagnostic clarity | Specific assessment of bulging disc vs other pain generators | Prevents treating the wrong driver |
| Defined outcomes | Pain/function baseline and measurable targets | Lets you judge response objectively |
| Adjunct plan | Rehab and load management running concurrently | Disc pain requires mechanical solutions too |
| Safety oversight | Clinical monitoring and risk screening | Reduces preventable complications |
| Evidence realism | Understanding that direct bulging-disc RCT evidence is limited | Protects expectations and decision quality |
FAQ
Is there strong bpc 157 for bulging disc back pain evidence?
The direct, high-quality human evidence specifically for bulging disc back pain is limited. Most support comes from preclinical plausibility and broader healing/inflammation research rather than large, spine-specific randomized trials.
What results should I realistically track if I try BPC-157?
Track pain intensity, function (sitting/walking tolerance), sleep, and any neurologic symptoms (tingling/numbness/strength). Also track medication changes. Decide success or lack of benefit using your pre-set criteria and a time window agreed with your clinician.
Should bpc 157 replace physical therapy or rehab?
No. The most evidence-aligned approach is to treat peptides as an adjunct while continuing a structured rehab program focused on load tolerance, mobility, and strengthening that matches your symptoms.
Conclusion: Use BPC-157 Thinking—Without the Guesswork
BPC-157 is discussed for pain management and healing because preclinical work suggests possible effects on inflammation and tissue recovery. However, when it comes to bpc 157 for bulging disc back pain evidence, the spine-specific human data is not strong enough to treat as definitive. The practical way to handle that gap is to pair any peptide strategy with an adjunct plan built on measurable outcomes, professional oversight, and proven bulging-disc care.
Next step: Start a 2-week baseline log (pain, function, and neurologic symptoms), then review it with a qualified clinician to determine whether BPC-157 can be tested safely as an adjunct—using clear goals and stop criteria.
Discussion