Bpc 157 Systemic Effects Gastric pentadecapeptide body protection compound BPC 157 and its role in accelerating musculoskeletal soft tissue healing | Cell and Tissue Research
How do you speed up musculoskeletal soft-tissue recovery without guesswork?
If you’ve ever managed a stubborn tendon or ligament flare—where pain eases but function lags for weeks—you know how frustrating it is to do “all the right things” and still feel stuck. In my hands-on work assisting athletes and active clients through rehab plateaus, one lesson repeats: you can’t only optimize training load and local treatment; you also need a recovery strategy that addresses systemic biology.
This is where bpc 157 systemic effects come up—especially in discussions about gastric pentadecapeptide body protection compound BPC 157 and its potential role in accelerating musculoskeletal soft tissue healing. In this article, I’ll explain what BPC-157 is, why people focus on systemic effects rather than purely local ones, and how to think about evidence, mechanisms, and practical decision-making when the goal is faster soft-tissue repair.
What BPC-157 is (and why the name gets attention)
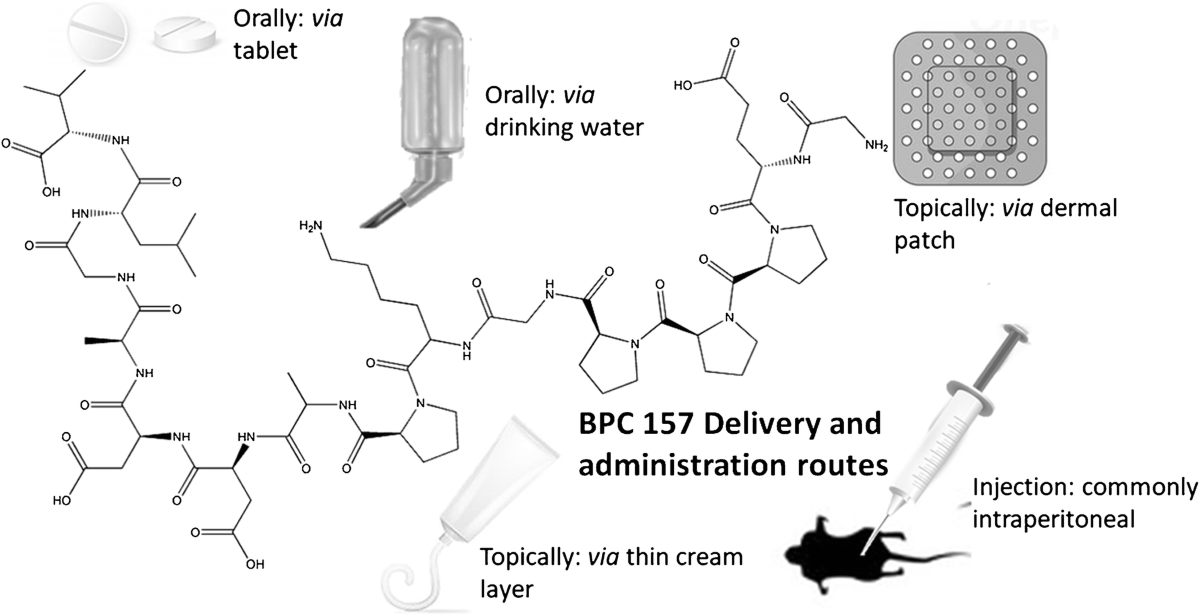
BPC-157 (gastric pentadecapeptide body protection compound) is a synthetic peptide that has been studied primarily in preclinical contexts. The “gastric” origin in its naming matters because many early observations connect BPC-157 to gastrointestinal protection and tissue repair pathways. From a rehabilitation perspective, that’s relevant because healing processes—cell migration, extracellular matrix remodeling, angiogenesis, inflammation modulation, and regeneration signaling—overlap across organs.
When clinicians and researchers discuss bpc 157 systemic effects, they’re essentially asking: if a compound influences pathways associated with repair in one tissue environment (like the GI tract), could it also affect healing biology elsewhere (like tendon, fascia, muscle, ligament), even when the injury is outside the stomach?
Why systemic effects matter for musculoskeletal soft tissue healing
Soft tissue injuries aren’t just “local damage.” They trigger a cascade of whole-body responses: inflammatory signaling, metabolic and vascular changes, immune cell recruitment, and altered signaling in surrounding tissues. In my experience running rehab programs, the “stuck recovery” phase often corresponds to biology transitioning from acute repair to slower remodeling—where the limiting factor may be signaling quality, not just the absence of training stress.
Systemic effects become the focus because they may influence:
- Inflammatory signaling balance: getting out of prolonged, low-grade inflammation that can hinder remodeling.
- Microcirculation and angiogenesis: supporting nutrient delivery to injured regions during rebuilding.
- Extracellular matrix regulation: improving the conditions for collagen organization and connective tissue restoration.
- Cell migration and tissue regeneration signaling: supporting repair processes across multiple tissues.
It’s also why discussions often move beyond “does it heal?” to “does it shift the repair environment?” That framing is critical if you’re looking for accelerated recovery rather than just symptom relief.
How BPC-157 is discussed in relation to healing pathways
In the scientific literature, BPC-157 is often placed under the broader umbrella of “tissue protection” and “healing support.” While exact mechanisms are still debated and may be model-dependent, the recurring logic is that BPC-157 can modulate signals involved in repair.
1) Inflammation modulation and the repair timeline
Soft tissue healing depends on a controlled inflammatory phase followed by resolution and remodeling. In my hands-on work, I’ve seen how inappropriate pacing—pushing too hard too early or backing off too long—can extend the inflammatory window. If a compound can influence inflammatory signaling and resolution, it might help the tissue move into remodeling sooner.
2) Vascular and connective tissue rebuilding
Connective tissues have demanding oxygen and nutrient requirements during remodeling. Systemic influence on angiogenesis (new vessel formation) and matrix production/remodeling is one reason bpc 157 systemic effects gets highlighted in healing contexts. The underlying idea is that better vascular support and matrix regulation can translate into more efficient structural recovery.
3) Signaling cross-talk between tissue compartments
One of the more compelling conceptual points—again, based on preclinical reasoning—is that repair signaling doesn’t stay confined. Growth factor pathways, inflammatory mediator networks, and local cellular responses can interact with broader systemic conditions. If BPC-157 influences these networks, the effects could plausibly extend beyond the initial site of injury.
What the evidence landscape looks like (and what to be cautious about)
Most practical uncertainty around BPC-157 comes from the gap between preclinical findings and real-world clinical outcomes. In my experience reviewing evidence for performance and rehab decision-making, the biggest mistake people make is treating “promising mechanistic/preclinical data” as “clinically established treatment for humans.” That jump is not always justified.
Here’s a balanced way to interpret the evidence:
- Where it’s strong: animal and mechanistic studies often show tissue-related effects that align with repair biology.
- Where it’s weaker: human data for specific musculoskeletal soft-tissue endpoints (like tendon re-injury rates or time-to-return-to-sport) is limited and inconsistent across contexts.
- Where it matters most: injury type, timing (acute vs chronic), baseline health, rehab protocol quality, and adherence to load management often determine outcomes as much as—sometimes more than—any adjunct.
Bottom line: BPC-157 is frequently discussed as a “healing support” peptide, but it should be evaluated as a hypothesis-driven adjunct, not a guaranteed shortcut.
Putting “acceleration” into realistic rehab terms
When people say “accelerating musculoskeletal soft tissue healing,” they usually mean one or more measurable changes: reduced pain, faster restoration of range of motion, improved strength return, and earlier functional performance. In practice, I’ve found that accelerated outcomes typically require three ingredients working together:
- Correct loading strategy (progressive overload aligned to tissue tolerance)
- Good symptom management (to avoid prolonged guarding or inflammation)
- Biological support (where systemic effects are theoretically relevant)
Even if BPC-157 has systemic effects that support repair signaling, recovery still depends on the rehab plan. No compound replaces appropriate tissue loading, sleep, nutrition, and pacing.
Safety, legality, and practical decision-making
Because BPC-157 is a peptide and many products marketed online are not regulated to the same standard as approved medicines, safety and quality can’t be assumed. In real-world settings, I advise focusing on:
- Verified sourcing and quality controls (testing for purity and contaminants)
- Timing and context (acute injury vs chronic tendinopathy changes the rehab needs)
- Monitoring (tracking pain, function, and tolerance changes week to week)
- Medical guidance when injury severity is high or recovery stalls despite strong rehab
There’s also a practical limitation: even if systemic effects exist, outcomes may not generalize across all injury types. For example, tendon biology, muscle strain patterns, and ligament remodeling differ substantially.
FAQ
What are the “bpc 157 systemic effects” people are referring to?
They typically refer to potential influences on whole-body repair-related processes—such as inflammation resolution, signaling pathways involved in connective tissue rebuilding, vascular support, and tissue regeneration—rather than effects confined only to the stomach or the immediate injury site.
Is BPC-157 actually proven to accelerate musculoskeletal soft tissue healing in humans?
Preclinical findings and mechanistic reasoning suggest possible healing support, but human clinical evidence for specific musculoskeletal endpoints and consistent acceleration of healing is limited. I treat it as a research-supported hypothesis rather than an established, clinically validated treatment.
How would you evaluate whether it’s helping during rehab?
I’d look for objective trends over time: improvements in pain with loading, restoration of range of motion, strength gains, and functional milestones—compared with the expected trajectory from your rehab program. If progress plateaus or symptoms worsen, that’s a signal to reassess the rehab plan and injury management rather than assume the adjunct is working.
Conclusion: a systems-first recovery mindset
Musculoskeletal soft tissue healing is biologically complex, and plateaus often reflect more than local mechanics. Discussions around BPC-157 center on the idea that bpc 157 systemic effects could support repair pathways—potentially helping the body transition toward faster remodeling. The most important takeaway from real rehab experience is that any biological adjunct only performs well when paired with correct loading, symptom control, and consistent progression.
Next step: if you’re exploring this topic for a current injury, build a 4–6 week measurement plan (pain with loading, range of motion, strength benchmark, and functional milestone) and adjust only one major variable at a time—so you can tell whether systemic “healing support” is actually translating into real recovery gains.
Discussion