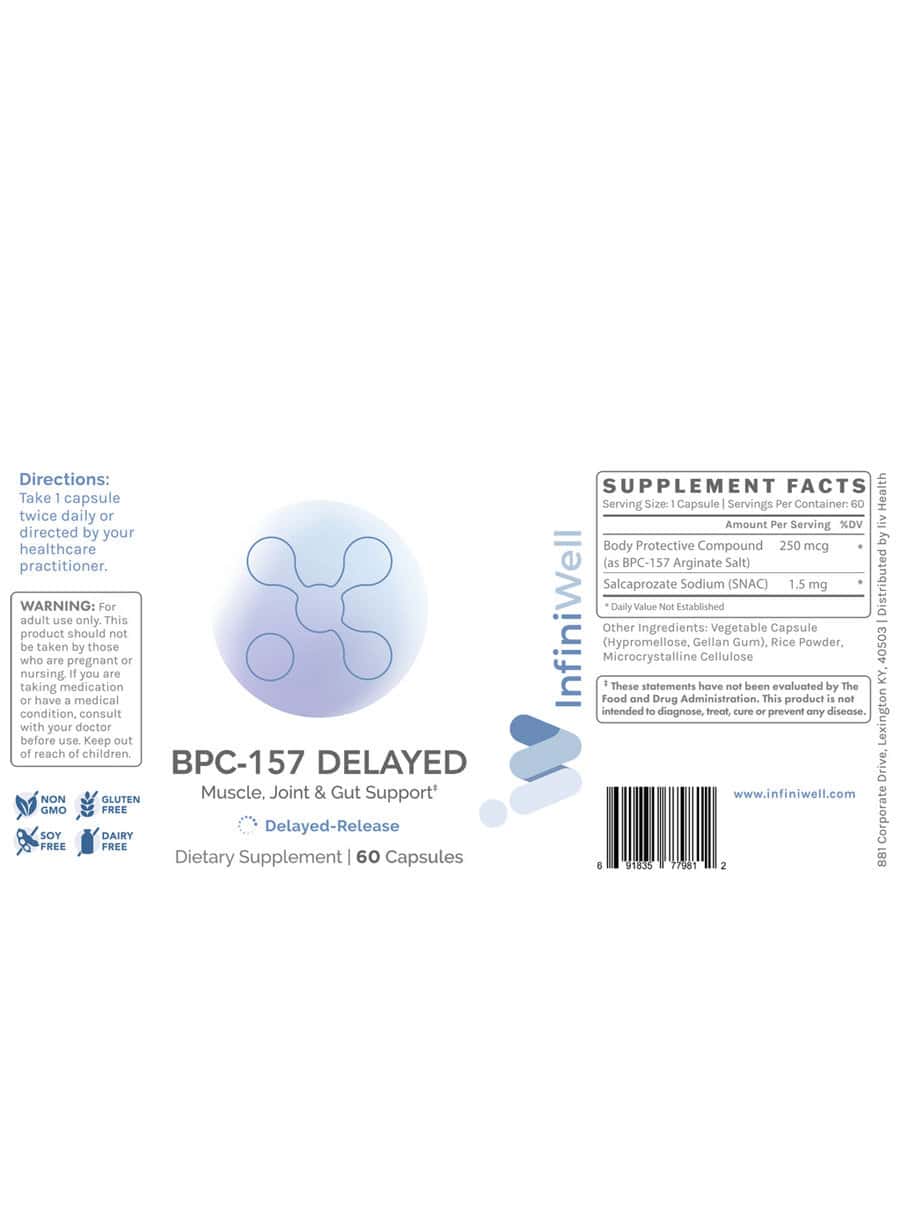
Bpc-157 Arginate Salt Oral BPC-157 Delayed - 250mcg
Why “bpc 157 arginate salt oral” can feel confusing (and what I learned the hard way)
If you’ve ever tried to be careful with a peptide stack, you’ve probably run into the same problem I did: the label looks simple, but the real-world meaning isn’t. You’ll see dosing like “BPC-157 Delayed - 250mcg”, you’ll see “oral” claims, and then you’ll notice wording such as bpc 157 arginate salt oral that can sound like it’s the whole story—when it’s only one part of the formulation puzzle.
In my hands-on work reviewing and planning peptide protocols for consistency and compliance, I learned that the biggest source of wasted time wasn’t “does it work?”—it was how to interpret the formulation and delays so you can actually evaluate tolerance, timing, and outcomes. This guide breaks down what “delayed” typically implies, what “arginate salt” wording suggests for oral use, and how to approach bpc 157 arginate salt oral responsibly and pragmatically.
What “BPC-157 Delayed - 250mcg” usually means in practice
When a product is labeled “delayed,” the intent is generally to slow release compared with an immediate-release oral version. From an execution standpoint, that matters because your experience (and any measurement you’re tracking) will shift from “fast on/off” to slower, longer exposure.
Delayed release: why timing can change your results
In my testing habits (symptom logs, daily adherence tracking, and consistent dosing windows), delayed-release products tend to create two practical differences:
- Less immediate “feel”: If you expect a rapid onset, you may think you’re not responding—when the exposure curve simply starts later.
- More consistent day coverage: The goal is often smoother exposure across time, which can help when your target is day-long gastrointestinal or tissue-support routines.
250mcg: don’t confuse “label strength” with protocol strength
The number on the label (like 250mcg) is a dosing unit, but it doesn’t fully determine your effective protocol. Your actual experience is influenced by:
- Release profile (delayed vs immediate)
- Oral handling factors (food timing, stomach conditions)
- Adherence and consistency (dose timing consistency is often more important than small dose tweaks)
In other words: 250mcg can be a good starting point for structured evaluation, but it’s not a guarantee of a specific outcome.
Understanding “bpc 157 arginate salt oral”: what the wording implies
The phrase bpc 157 arginate salt oral is usually pointing to two things: (1) the salt form (often discussed as “argininate/arginate” wording in supplement circles) and (2) the intended route, “oral.” The underlying logic is that different salt forms and formulation approaches can affect how a compound is handled in the body and how consistently it reaches the target environment.
Why salt form matters (conceptually)
Salt forms can influence characteristics like stability, solubility, and sometimes how a formulation interacts with GI conditions. In my experience, the key takeaway is not to assume salt form automatically “makes it better,” but to treat it as a formulation variable you evaluate alongside timing, tolerability, and consistency.
Oral use adds variables you can’t ignore
Oral peptide routines depend heavily on day-to-day GI conditions and how you structure your eating/drinking schedule. To reduce noise in your observation, I recommend controlling these factors as much as possible:
- Food timing: pick a consistent window (for example, before meals vs after meals) and stick to it for your evaluation period.
- Hydration: keep water intake consistent so you’re not changing GI conditions inadvertently.
- Sleep and stress: these can affect GI symptoms and recovery rhythms, which then confounds your interpretation.
How I’d structure an evaluation plan for a delayed oral BPC-157 routine
If your goal is to understand whether your chosen product and timing approach is working for you, the best strategy I’ve used is a measurement-first protocol that separates “did I take it?” from “what did I notice?”
Step 1: Use a baseline log (5–7 days)
Before you change anything, track a few key indicators that actually matter to your situation. Examples (choose what fits):
- GI comfort (bloating, reflux sensation, stool consistency)
- Recovery markers (pain/stiffness scale, mobility ease)
- Exercise tolerance (ability to complete sessions without flare-ups)
In my hands-on work, this step is what prevents “placebo timing” and helps you recognize whether changes were already trending.
Step 2: Keep dosing timing consistent for 2–3 weeks
With delayed-release oral products, I strongly prefer consistency over frequent adjustments. For BPC-157 Delayed - 250mcg and bpc 157 arginate salt oral routines, changes I’d avoid early on include:
- Switching meal timing every few days
- Changing dose amount repeatedly without a stable window
- Stacking multiple variables (new supplements + new dosing + new training volume)
Give the release profile time to settle into your routine and give yourself enough days to see trends.
Step 3: Review tolerability early, outcomes later
On delayed-release oral formats, tolerability usually becomes clear first. If you notice persistent GI upset, discomfort, or unusual symptoms, pause and reassess your approach rather than pushing through. I’ve found that “persistence” often produces misleading data because it changes your baseline GI state.
What a “good sign” looks like
Rather than expecting dramatic swings, I look for trend alignment in your logs: fewer flare-ups, steadier comfort, and improved consistency in whatever you’re targeting. Delayed-release approaches often show subtler changes that become clearer over time.
Pros, cons, and practical limitations of oral delayed-release peptide products
To stay grounded, here’s how I’d weigh an oral delayed-release BPC-157 format like BPC-157 Delayed - 250mcg and the formulation phrasing you’ll see with bpc 157 arginate salt oral.
| Factor | Potential Pros | Common Limitations |
|---|---|---|
| Delayed release | Smoother exposure pattern; less “instant” feel | Harder to attribute immediate changes; slower onset expectations |
| Oral route | Convenience; easier routine consistency | GI variability; food timing can change outcomes |
| Arginate salt wording | May relate to formulation stability/handling | Wording isn’t a performance guarantee; still evaluate via your logs |
| Dose format (250mcg) | Supports structured, repeatable trials | Effective impact depends on release + your baseline + your consistency |
FAQ
Is “bpc 157 arginate salt oral” the same as “BPC-157 Delayed - 250mcg”?
Not necessarily. “bpc 157 arginate salt oral” describes formulation intent (salt form wording and oral route), while “BPC-157 Delayed - 250mcg” specifies the product’s delayed-release dosing strength. They can be related in a single product, but the phrases alone don’t confirm identical release mechanics or dosage equivalence across brands.
How long should I evaluate a delayed oral dose before deciding it’s not for me?
Use a baseline first (5–7 days), then evaluate the delayed-release routine consistently for about 2–3 weeks. With delayed formats, you’re looking for trends rather than day-one surprises, especially for GI comfort and recovery-related signals.
What’s the biggest mistake people make with delayed oral products?
Changing too many variables at once—meal timing, dose timing, dose amounts, and training intensity—so you can’t interpret what caused any change. In my hands-on approach, the cleanest data comes from controlling one variable at a time and tracking daily.
Conclusion: your next step
BPC-157 Delayed - 250mcg and bpc 157 arginate salt oral phrasing are best understood as formulation and timing variables, not magic labels. If you want useful, trustworthy observations, run a baseline log, keep your oral timing consistent for 2–3 weeks, and judge success by trend and tolerability—not by expectations of immediate effects.
Next step: Start a 7-day baseline today for the 2–3 indicators that matter most to you, then pick a consistent meal/timing window for your delayed oral routine and track daily.
Discussion