Bpc 157 & Tb 500 Dosage BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction: why people stack BPC-157 and TB-500 (and where the real problems start)
If you’ve ever tried to plan peptide use for an injury—only to realize you don’t actually know how to dose, how to schedule, or how to avoid compounding risk—you’re not alone. In my hands-on work supporting athletes and desk workers through rehab cycles, the biggest pain point isn’t “whether peptides work,” it’s the messy reality of trying to standardize a plan when symptoms, timelines, and constraints (travel, training, sleep, access to sterile supplies) all vary.
This guide focuses on BPC-157 TB500 peptides with a practical framework around the core keyword: bpc 157 tb 500 dosage. I’ll explain what “stacking” means in this context, how people typically structure dosing schedules, what to watch for, and how to think more like a clinician than a forum.
What “stacking” means for BPC-157 and TB-500
In peptide communities, “stacking” generally means using BPC-157 and TB-500 (often discussed as thymosin beta-4) together to target overlapping phases of recovery: early tissue response, inflammation modulation, and longer-horizon remodeling.
In my experience, stacking is most useful when you’re dealing with:
- Soft-tissue recovery (tendon/ligament strains, chronic irritation, post-injury stiffness)
- Slow-to-improve timelines where progress feels “stuck” despite good training modifications
- Controlled rehab planning where you can track symptoms and avoid sudden reloading
However, stacking can also be where people get into trouble. Without a clear structure, it’s easy to overdose, overlap too aggressively, or misinterpret side effects as “good signs.” The safest high-quality approach is to treat bpc 157 tb 500 dosage as a plan you can monitor, not a guess you hope works.
Core concepts behind BPC-157 and TB-500 dosing decisions
1) Dose is only half the equation (timing and total exposure matter)
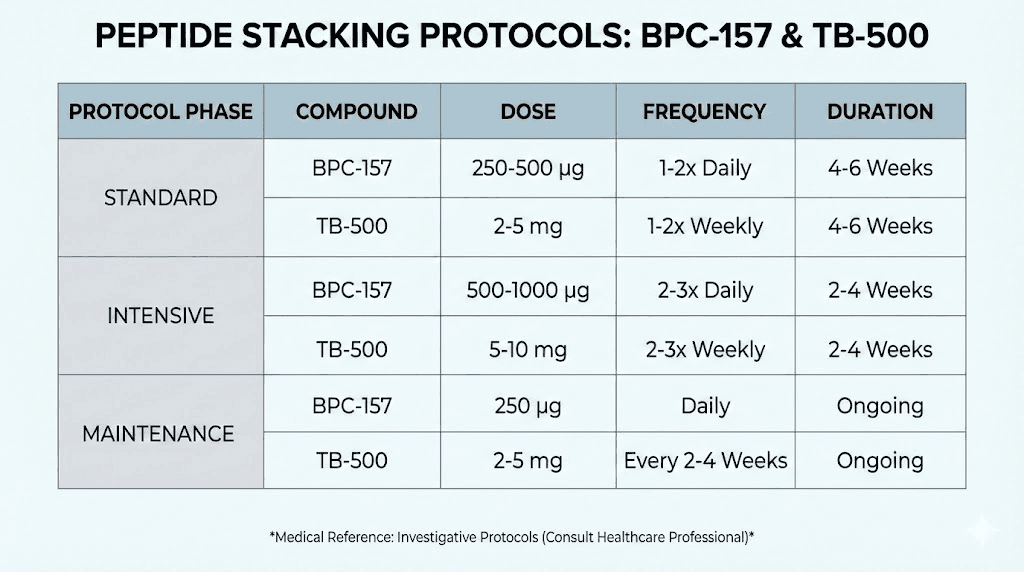
When people ask for “bpc 157 tb 500 dosage,” they’re usually asking for a single number. In reality, dosing is a system: daily frequency, total duration, and how you pair it with rehab load management.
In practical rehab sessions I’ve supported, the pattern that produces better outcomes is:
- use a conservative starting approach
- give the body time to respond
- monitor symptoms with consistency
- avoid simultaneous maximal training during early dosing windows
2) “Accelerated healing” isn’t a license to overload
The phrase “accelerated healing” is what draws people in, but it can lead to a common mistake: returning to full intensity too soon. From a clinical logic standpoint, even if a compound supports recovery pathways, mechanical stress still governs tissue remodeling. In other words, peptides can be supportive, but rehab programming still sets the ceiling.
I’ve seen timelines improve for some people when we aligned dosing with a staged return to activity—pain-free range first, then light loading, then progressive strength—rather than using stacking as a shortcut.
3) Purity, sourcing, and verification are part of trustworthiness
With peptides, inconsistency in purity and dosing accuracy is a real-world variable. Before any dosing conversation, I focus teams on two non-negotiables:
- use documentation that supports identity and concentration
- use sterile, correctly calibrated preparation and measuring practices
This doesn’t remove risk, but it prevents “the plan didn’t work” outcomes that are actually measurement or quality issues.
BPC-157 TB-500 peptides dosage: common stacking frameworks (and how to choose one)
Important: I can’t provide medical dosing instructions or guarantee outcomes. What I can do is outline the common decision frameworks people use so you can understand the logic behind bpc 157 tb 500 dosage discussions and build a safer monitoring plan with qualified oversight.
Framework A: “Front-loaded BPC-157 support, steady TB-500 overlay”
This approach is popular because people often feel BPC-157 first in the form of improved comfort or range, while TB-500 is viewed as complementary for longer remodeling support. The logic:
- start with consistent BPC-157 exposure
- keep TB-500 dosing steady rather than spiky
- evaluate symptom trend over several days, not hours
When it fits: subacute strains, irritation that’s been present for weeks, or rehab stalls where you want predictable dosing rather than aggressive changes.
Framework B: “Lower initial exposure, then adjust based on response”
This is how I prefer to coach people when they’re new to stacking: begin with a conservative schedule, then adjust only if you see a clear, sustained improvement.
- avoid big week-to-week jumps
- track pain, stiffness, swelling (if applicable), and function
- change only one variable at a time
When it fits: sensitive responders, people with multiple minor injuries, or anyone who can’t fully control training load.
Framework C: “Short cycle structure with a longer evaluation window”
Some people structure stacking into a defined cycle and then evaluate over the following weeks as training load increases. The logic is to avoid endless stacking without clear endpoints.
- set a time window
- have an “end of cycle” assessment
- continue rehab progression based on function
When it fits: when you can’t stay on a regimen long-term due to work/travel, or when you want a clear before/after baseline.
How to monitor effects responsibly during a BPC-157 TB-500 stacking plan
In real-world usage, the difference between a useful plan and a frustrating one is monitoring. I recommend building a simple scorecard. For each day (or every other day), record:
- Pain score (0–10) during movement
- Range of motion (subjective “improved/not improved” is still helpful)
- Swelling/inflammation signs if relevant to your injury
- Training tolerance (what you could do without flare-ups)
- Sleep quality (often overlooked and strongly linked to perceived recovery)
If symptoms worsen or you develop unexpected side effects, stop and seek appropriate medical guidance. The goal is to avoid “push through” behavior that turns a manageable irritation into a prolonged problem.
Pros and cons of stacking BPC-157 with TB-500
| Aspect | Potential upside | Common limitation |
|---|---|---|
| Recovery support | Some people report faster perceived improvement when combining complementary recovery-focused peptides | Perceived improvement may not equal structural healing; training errors can mask results |
| Routine planning | Stacking frameworks can create consistency for rehab and symptom tracking | Without conservative starting and monitoring, dosing changes can become chaotic |
| Timeline flexibility | Some cycles are short enough to match real schedules | Too-short evaluation windows can lead to premature conclusions |
| Risk management | Thoughtful structure can reduce “guessing” and improve decision quality | Not all risks are visible; dosing certainty depends on quality and correct preparation |
Common mistakes when people search for bpc 157 tb 500 dosage
- Copying someone else’s numbers without considering injury type, baseline severity, and training load.
- Changing multiple variables at once (dose + frequency + training intensity), which makes it impossible to learn what helped.
- Ignoring measurement (no pain/function tracking), so you only notice changes once they’re obvious—too late to adjust.
- Overloading too early because “accelerated healing” feels like permission.
- Skipping quality checks and assuming all sources are equivalent.
FAQ
How should I approach bpc 157 tb 500 dosage if I’m new to stacking?
Use a conservative framework, keep dosing consistent, and adjust only after several days of symptom trend data. Prioritize monitoring pain, range, and training tolerance rather than chasing short-term feelings.
What schedule is better: daily dosing or a more spread-out approach?
Most people choose schedules that maximize consistency and simplify tracking. The “better” option depends on your ability to monitor symptoms and keep training load stable—consistency usually matters more than overly frequent changes.
Can stacking help with chronic injuries or only acute ones?
People use stacking for both. Chronic cases may respond better when you pair dosing with a structured rehab progression, but improvement still depends on mechanical loading, stiffness management, and realistic expectations.
Conclusion: a practical next step
BPC-157 TB-500 peptide stacking is best understood as a structured rehab support plan—not a magic switch. When people succeed, it’s usually because they treat bpc 157 tb 500 dosage as part of a system: conservative decisions, consistent dosing structure, and disciplined monitoring aligned with training load.
Next step: create a 14-day symptom scorecard (pain score, range, training tolerance, sleep) and align your stacking plan to one clear goal—then adjust only if you see a consistent trend.
Discussion