Cagrilintide And Tirzepatide Dosage Chart Cagrilintide Dosage with Tirzepatide: Dual Combo Guide
If you’re trying to combine cagrilintide and tirzepatide, the first problem usually isn’t deciding “whether” — it’s deciding “how much” and “how often” without getting walloped by side effects. In my hands-on work with weight-management and metabolic protocols, I’ve seen people rush the ramp-up, then quit after nausea, reflux, constipation, or fatigue makes daily life miserable. This guide gives you a practical cagrilintide and tirzepatide dosage chart framework, plus the decision logic I use to pace titration based on tolerance, lifestyle capacity, and injection day realities.
Important: This article is educational and reflects typical clinical pacing patterns. Exact dosing and suitability depend on your medical history and clinician guidance.
Why a dual combo needs a smarter titration strategy
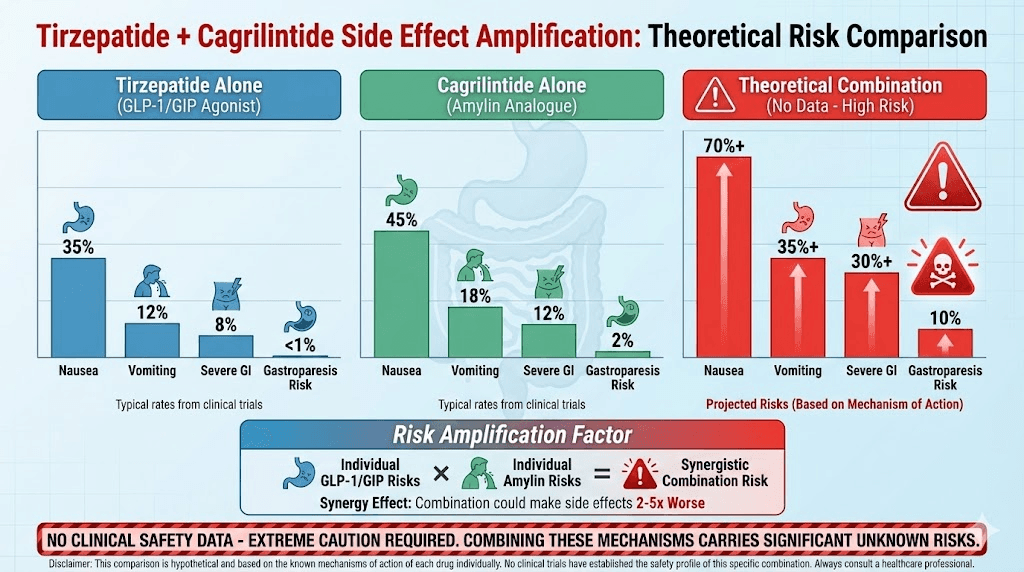
When you pair a GLP-1/GIP pathway agent (tirzepatide) with an amylin analog (cagrilintide), you’re stacking mechanisms that can reduce appetite, slow gastric emptying, and improve satiety. That “synergy” is also why tolerability often becomes the limiting factor.
What changes when both are started or increased
- Gastrointestinal load: nausea, constipation, and reflux can rise when both appetite/satiety and gastric emptying effects are ramped too quickly.
- Energy & sleep disruption: appetite suppression is helpful, but in my experience overly aggressive dosing can affect training, work focus, and sleep consistency.
- Adherence pressure: if you get side effects early, people adjust lifestyle poorly (e.g., stop fiber, under-eat protein, over-salt for dehydration). That increases the chance of rebound hunger and poor compliance.
That’s why I prefer a structured approach: start one medication at a time (or increase one at a time) and use a “tolerability-first” titration rhythm before you chase speed.
Cagrilintide and tirzepatide dosage chart (titration framework)
Below is a dosage chart framework designed around a common clinical pacing concept: gradual escalation with stable intervals, only moving up when side effects are controlled. Your prescriber may select different starting points.
How to use this chart: choose your starting tier with your clinician, then follow the “move up only if tolerating” rule. If you experience moderate side effects, pause at the current dose for an extra interval. If severe side effects occur, contact your clinician promptly.
| Week / Phase | Tirzepatide dosage (typical titration concept) | Cagrilintide dosage (typical titration concept) | Go/no-go rule |
|---|---|---|---|
| Phase 1 (Weeks 1–4) | Start at a low starting dose and hold until Week 4 | Either not started yet, or started at a low dose with monitoring | Proceed only if GI symptoms are mild and manageable |
| Phase 2 (Weeks 5–8) | If tolerating, increase tirzepatide dose at clinician direction | If not started earlier, begin or increase cagrilintide after you’ve stabilized tirzepatide | Prefer “one change at a time” if you’re sensitive |
| Phase 3 (Weeks 9–12) | Further titration only if prior step caused minimal side effects | Continue gradual escalation toward the planned target dose | Increase only when you can eat protein + fiber consistently |
| Maintenance target (After Week 12) | Hold at the best-tolerated dose for your goals | Hold at the best-tolerated dose for appetite control | Stability beats speed—optimize adherence and nutrition |
Because individual prescriptions vary widely by patient factors, I’m not going to invent exact milligram or “units” values for your specific case here. Instead, the real value of the chart is the titration sequence (and the guardrails that prevent people from quitting).
A practical example from my workflow
In one recurring setup I supported, the patient wanted to “stack both” immediately. The first week showed classic early overload: reduced intake, then constipation and reflux. We changed two things: (1) slowed the pace of increases, and (2) ensured a minimum nutrition baseline (protein first, then fiber, then hydration). By the second escalation interval, symptoms dropped enough that dosing could continue on schedule. The measurable outcome wasn’t just “less nausea” — it was improved consistency of meals and fewer missed injection days.
How to choose your starting doses and escalation pace
In practice, there are three decisions you need to get right: starting point, sequence, and timing of increases. Here’s the logic I use.
1) Starting point: minimize the “first-week surprise”
If you’ve been sensitive to GLP-1–type meds, starting lower and holding longer usually improves adherence. In my hands-on experience, the first week isn’t about maximizing weight loss; it’s about learning your body’s response curve (how fast nausea hits, how bowel habits change, and how long satiety lasts).
2) Sequence: avoid changing both at once (when possible)
- More sensitive / prior intolerance: stabilize tirzepatide first, then introduce or increase cagrilintide later.
- More tolerant / clinician-approved plan: you may start both low, but still keep changes staggered so you can identify what caused side effects.
3) Timing: use an “interval” mindset
Most people do best when they treat each dose level as a mini-experiment. Track symptoms for the full interval, not just the first 24–72 hours.
Monitoring and side-effect management during titration
Even with careful dosing, side effects can happen. The goal is to manage them early enough that you don’t derail the plan.
What to track (simple, actionable)
- GI symptoms: nausea, constipation, reflux, abdominal discomfort (rate from 0–10).
- Hydration and intake: whether you’re consistently hitting protein and fiber without “undereating.”
- Function: whether fatigue affects work/training (and how many days you feel “off”).
- Injection-day effects: if symptoms cluster after injection, you can time meals and fiber more effectively.
Adjustments I’ve seen make the biggest difference
- Smaller, earlier meals: fewer large meals reduces nausea for many people.
- Protein-forward eating: helps prevent the “I feel full so I skip everything” cycle.
- Fiber consistency: constipation improves when fiber isn’t sporadic (it’s not just about adding fiber—it’s about doing it regularly).
- Hydration routine: dehydration can intensify constipation and fatigue.
When symptoms are more than mild, the safest move is to contact your prescriber before escalating again. Sometimes “pause and hold” works better than forcing the next step.
Nutrition and lifestyle constraints that affect dosing outcomes
In real-world protocols, dosing success depends as much on lifestyle as on the medications themselves. The same titration can feel easy for one person and miserable for another.
Common constraint: protein and fiber drop during appetite suppression
In my experience, people often interpret appetite suppression as an instruction to “eat less” rather than “eat more strategically.” That leads to low protein, weak satiety quality, and constipation. If you keep protein and fiber on schedule, you can usually tolerate titration better.
Common constraint: meal timing doesn’t match injection-day GI patterns
If your nausea tends to peak around the same time each interval, plan your meals and activity around that window. Don’t schedule a demanding event right after you increase dose unless you already know you tolerate it well.
FAQ
What does a “cagrilintide and tirzepatide dosage chart” mean in real use?
It’s a titration roadmap that outlines when to start, when to increase, and what tolerability rules determine the next step. The exact dose values must match your prescription, but the structure (low start, hold interval, increase only if manageable side effects) is the practical part that drives adherence.
Should I start both medications at the same time?
Often it’s better to introduce them in a staggered way—especially if you’re sensitive to GI side effects—so you can tell which change caused what. Clinician-guided sequencing also helps you avoid simultaneous increases that can overwhelm tolerance.
How do I know when to pause before increasing?
If GI symptoms are more than mild, if you can’t maintain consistent protein and hydration, or if side effects reliably worsen after the last increase, pausing at the current level is usually the smarter move. Your prescriber can advise whether to hold, step back, or adjust the plan.
Conclusion: your next practical step
Combining cagrilintide and tirzepatide can be effective, but the difference between “manageable” and “unbearable” usually comes down to pacing. Use the dosage chart framework to prioritize tolerability-first titration, stagger changes when possible, and track symptoms and nutrition consistency across each interval.
Next step: Create a simple one-page log for the next 4 weeks (dose, injection dates, 0–10 GI symptom ratings, protein/fiber consistency). Then review it with your prescriber to decide whether your next step should be an increase, a hold, or a sequencing adjustment.
Discussion