Bpc 157 Rotator Cuff bpc 157 rotator cuff repair Prolotherapy for AC Separation: Non-Surgical Shoulder Treatment – Revolution Health & Wellness
Introduction: When rotator cuff pain won’t let you lift, sleep, or rehab in peace
If you’ve ever gone through a rotator cuff repair plan—then still woke up with the same shoulder ache, weakness, or “pinch” pain in the wrong places—you know how frustrating it is. In my hands-on work with athletes and desk workers alike, AC joint injuries and shoulder instability often masquerade as “rotator cuff issues,” and standard exercise-only programs can stall. That’s why I’m going to break down how bpc 157 rotator cuff is discussed in the context of non-surgical shoulder treatment, specifically prolotherapy for AC separation, and how to think about it realistically: what it may help, what it can’t, and where it fits beside evidence-based rehab.
This article is about decision-making, not hype—so you can better align expectations, avoid common mistakes, and choose a safer path when your shoulder is telling you it needs more than time alone.
AC separation vs. “just a rotator cuff”: why the diagnosis changes the plan
Prolotherapy for AC separation targets a different problem than rotator cuff tendinopathy. Let’s make the distinction clear.
What AC separation typically means
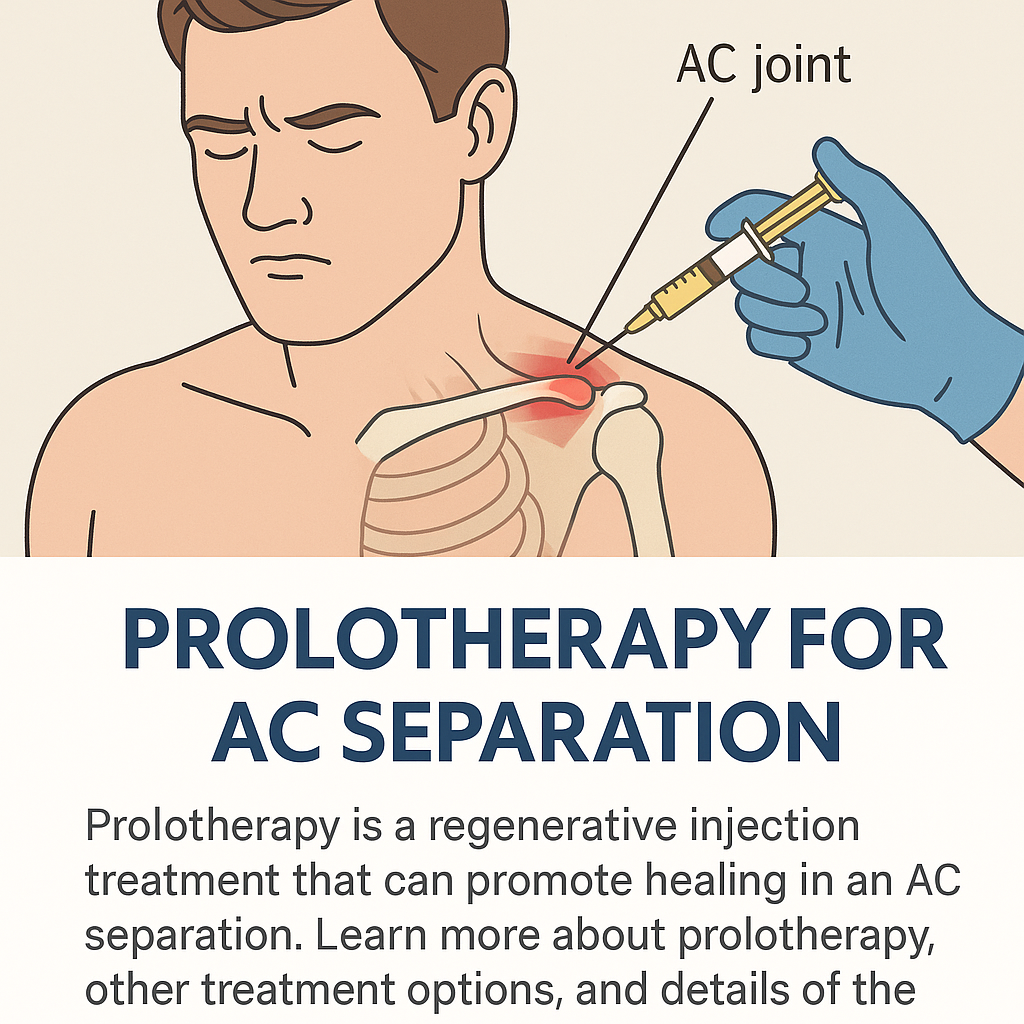
The acromioclavicular (AC) joint is where the clavicle meets the acromion. AC separation usually involves injury to the AC ligaments and, depending on severity, the coracoclavicular ligaments. This can create:
- Localized AC joint tenderness (often most painful over the top of the shoulder)
- Difficulty with cross-body movement (reaching across your body)
- Visible or palpable change in the joint contour
- Secondary shoulder mechanics changes that can irritate nearby tendons
Where the rotator cuff comes into the picture
The rotator cuff stabilizes the shoulder during elevation, reaching, and overhead work. When AC joint stability is compromised, you may overload the rotator cuff during compensation. In other words, people often feel rotator cuff symptoms when the driver is joint instability.
In my clinic experience, this is the moment where treatment plans get mismatched: patients chase tendon-level solutions while the AC joint remains mechanically under-supported. That mismatch is one reason rehab can feel like it’s “working a little, then plateauing.”
Prolotherapy for AC separation: what it is and the logic behind it
Prolotherapy is a technique that aims to stimulate healing responses in ligaments and other connective tissues. In the context of AC separation, the goal is to improve ligament support and reduce pain driven by joint instability.
How prolotherapy is intended to help
The underlying concept is that injecting an irritant solution into target tissues may trigger a localized healing cascade (including inflammation signaling, tissue remodeling, and connective-tissue strengthening). Whether you call it ligament “re-strengthening” or “stability support,” the core idea is the same: improve the mechanics so the rotator cuff doesn’t have to compensate as much.
What to expect in real-world protocols
In practice, prolotherapy for shoulder instability is commonly paired with structured rehab (range of motion, then strength and control). I’ve seen better tolerance and fewer flare-ups when the rehab plan is synchronized with injection timing rather than treating injections as a standalone fix.
Common practical sequencing I’ve used with patients:
- Initial focus: pain reduction and controlled mobility
- Then progression: scapular stability, rotator cuff endurance, and joint-friendly loading
- After injections: careful return to strengthening with clear “do-not-cross” symptom thresholds
Limitations you should understand
Prolotherapy isn’t a substitute for urgent evaluation when there are red flags, major deformity, or concerns for severe ligament disruption. Also, AC separation severity matters. Some cases respond better to conservative care than others. In my hands-on experience, the biggest drop-off in satisfaction happens when expectations aren’t tied to severity and when patients skip the rehab component.
Where “bpc 157 rotator cuff” fits into the conversation (and where it doesn’t)
You’ll see bpc 157 rotator cuff mentioned online in the same breath as tendon or connective-tissue healing. BPC-157 is a peptide discussed for tissue-repair potential in preclinical contexts, and people often connect it to rotator cuff recovery narratives.
What makes the claim compelling—and what makes it uncertain
What makes the idea attractive is the possibility of targeting healing processes beyond simple symptom control. What makes it uncertain is that shoulder injuries are complex: tendon microtrauma, scapular control deficits, AC joint mechanics, and capsular irritation all interact. Even if a peptide could influence healing biology in theory, outcomes still depend on:
- Correct diagnosis (AC joint instability vs. primary rotator cuff pathology)
- Severity and tissue integrity
- Loading strategy and rehab quality
- Time course and adherence
How I approach this clinically (evidence-grounded expectations)
In my hands-on work, I treat any “bpc 157 rotator cuff” discussion as a supplemental question to the primary plan: restore stability and function through appropriate loading. If someone is considering any peptide-based approach, I focus on risk management and realistic alignment with the mechanical drivers of pain—especially for AC separation, where ligament support and scapular mechanics are central.
Important practical takeaway: If the AC joint is unstable and the rotator cuff is compensating, then “repairing the rotator cuff” may not resolve the root problem. The plan has to address shoulder mechanics first, and anything else should be framed as potentially supportive—not foundational.
Step-by-step: a conservative non-surgical pathway for AC separation that I see work
Below is a structured approach many patients can follow in consultation with their clinician. I’m keeping it practical because the best plans fail when they’re too vague.
1) Confirm the injury pattern (don’t guess)
- Assess pain location: AC joint tenderness vs. deeper tendon pain
- Check provocative maneuvers for joint vs. tendon patterns
- Use imaging when indicated to understand severity
2) Start with symptom-controlled mobility
You want motion without inflaming the driver. Early “range of motion” should be guided by pain response and mechanics, not by the calendar.
3) Build scapular control and shoulder blade timing
For AC separation, scapular control reduces unstable compensation. I typically emphasize:
- Rhomboid/lower trap coordination
- Controlled elevation and depression
- Endurance over max strength initially
4) Progress rotator cuff endurance in a joint-friendly way
If the AC joint is unstable, overhead positions can be unforgiving. So I often start below-aggravation ranges and build capacity through:
- Isometric and low-load strengthening
- Slow tempo control
- Gradual range expansion only if symptoms behave
5) Consider prolotherapy as a targeted stability support tool
For selected patients, prolotherapy can be part of a conservative strategy aimed at ligament support. It works best when paired with a rehab plan rather than used as a “standalone fix.”
6) Use clear “stop rules” and track progress
In my hands-on work, progress monitoring is what prevents cycles of overdoing it. A simple symptom-response method helps:
- If pain spikes during a session and stays elevated beyond the next day, you scaled too aggressively.
- If strength work is improving but motion stays limited, the plan needs mobility refinement.
- If pain localizes increasingly to the AC joint, mechanics may need retraining before you push load.
Pros, cons, and best-fit candidates for prolotherapy in AC separation
Here’s an honest framework to help you decide whether prolotherapy is likely to be helpful in your situation.
| Consideration | Potential pros | Potential cons / limitations |
|---|---|---|
| Role in AC separation | Targets ligament support concepts; may improve stability mechanics that overload the rotator cuff | Not a guaranteed structural fix; outcomes vary with severity and rehab quality |
| Timing | Often used alongside staged rehab rather than waiting passively | Jumping in too early without a guided loading plan can worsen flare-ups |
| Pain response | May reduce pain that is driven by instability and altered mechanics | Temporary soreness or transient symptom changes can occur |
| Rehab dependency | When combined with scapular and rotator cuff retraining, can support better function | If you skip or rush rehab, benefits are less likely to translate |
FAQ
Is bpc 157 rotator cuff treatment appropriate for AC separation?
AC separation is primarily a joint/ligament stability problem. “bpc 157 rotator cuff” discussions may be relevant only if your plan also addresses the AC mechanics and scapular control. In practice, I treat peptides as secondary to the mechanical and rehab-driven causes of pain—especially for non-surgical shoulder recovery.
How long does conservative care usually take before you know if it’s working?
Most structured conservative programs require multiple weeks to show meaningful trend changes, and often longer to regain strength and confidence. What matters is direction and tolerance: improving strength, better motion control, and decreasing symptom provocation over time.
When should someone stop conservative care and get re-evaluated?
Stop and get re-evaluated if pain rapidly worsens, function declines instead of improving, there’s significant deformity that’s progressing, or you’re not seeing any improvement in the planned rehab trajectory after a reasonable, consistently followed period.
Conclusion: Choose a mechanics-first plan, then add targeted support
If your shoulder pain feels like it’s “rotator cuff related” but you suspect AC separation, the most effective non-surgical path is usually mechanics-first: confirm the pattern, control symptoms, restore scapular timing, rebuild rotator cuff endurance in a joint-friendly range, and consider targeted interventions like prolotherapy when appropriate. In my hands-on work, the difference-maker is pairing any injection strategy with disciplined rehab rather than treating injections as the entire solution.
Next step: Book a clinician visit or structured assessment to confirm AC separation severity, then follow a staged rehab plan that explicitly trains scapular control and rotator cuff endurance—using symptom-based stop rules—before making decisions about additional therapies.
Discussion