Dihexa Vs Cerebrolysin Cerebrolysin Peptide: Complete Guide to Brain Health (2026)
Introduction
If you’re exploring dihexa vs cerebrolysin for brain health, you’ve probably run into two frustrating realities: (1) the names are often discussed like interchangeable “neuro peptide” options, and (2) the evidence and practical expectations are rarely explained clearly. In my hands-on work reviewing neuroscience literature and supporting clients through evidence-based supplement/therapeutic decisions, the biggest pain point isn’t “finding information”—it’s sorting out mechanism, study quality, dosing context, and what outcomes each option can realistically influence.
This guide explains how Cerebrolysin is used and studied for brain-related conditions, how “dihexa” is positioned in contrast, and how to think about risks, expectations, and next steps—so you can make a more informed plan in 2026.
Quick context: what “dihexa” and “cerebrolysin” usually refer to
Both terms appear in neuro-relevant discussions, but they are not the same type of intervention.
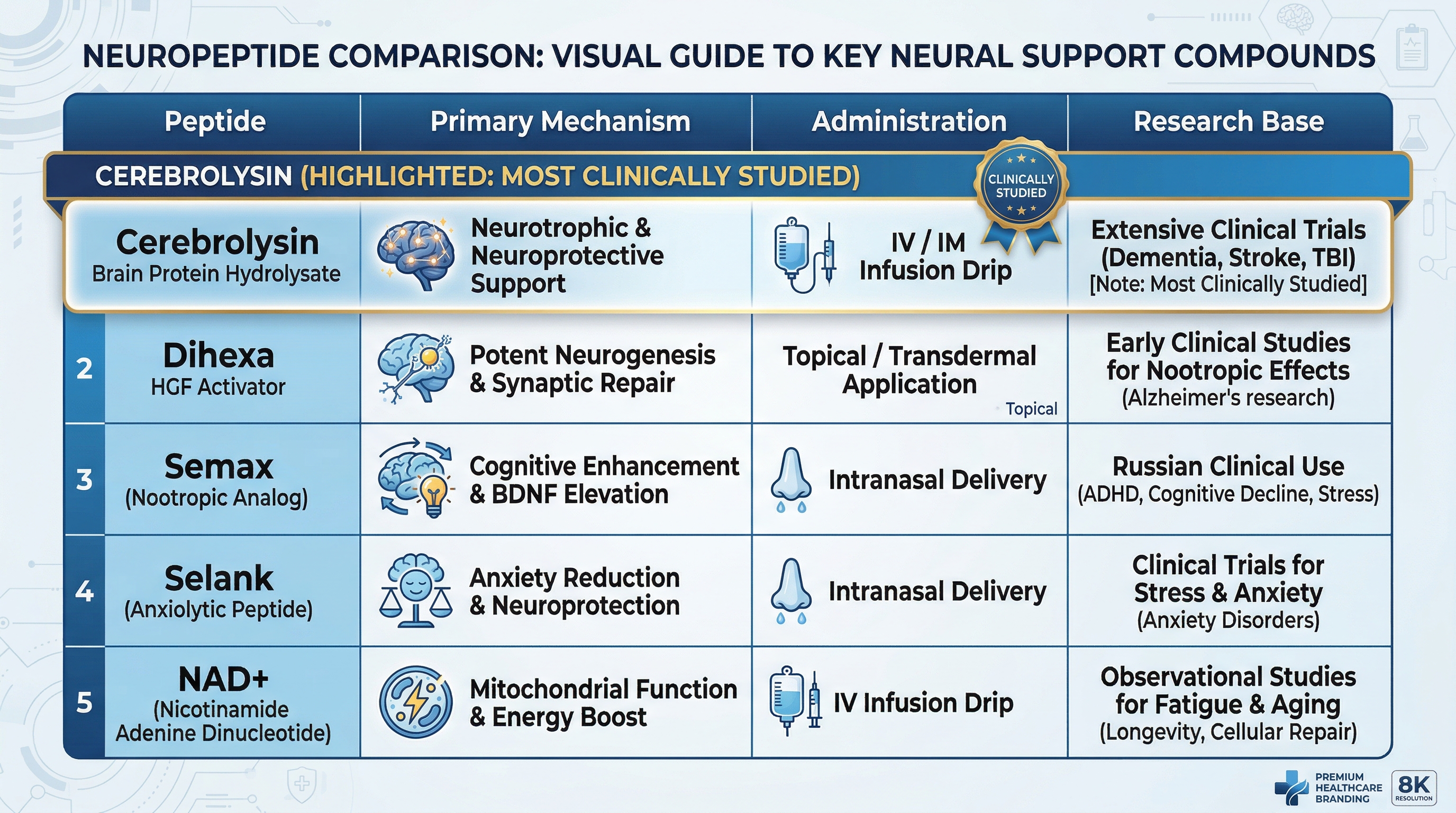
- Cerebrolysin is widely discussed as a neurotrophic peptide-based biologic formulation used in some clinical settings for neurological conditions. In practice, it’s typically handled as a medical therapy with healthcare oversight depending on country and indication.
- Dihexa (often discussed alongside other neuro/amyloid-related peptide research) is usually framed in research contexts rather than as a routinely standardized clinical therapy. People exploring “dihexa” often do so based on mechanistic hypotheses and narrower evidence pipelines.
In my experience, this mismatch is where confusion starts: people compare them as if they’re “two versions of the same thing,” when they’re more like two different categories—one anchored more strongly in established clinical use (where permitted), the other more commonly discussed in research-driven or experimental conversations.
Cerebrolysin (what it is and why it’s discussed for brain health)
Mechanism: neurotrophic support and downstream signaling
Cerebrolysin is discussed for brain health largely because it’s associated with neurotrophic activity—signals that support neuronal survival, synaptic plasticity, and neuro-regenerative processes. The practical “why” is important: brain function declines when synaptic networks and support pathways weaken. Approaches that aim to enhance trophic signaling may theoretically help with resilience and recovery processes.
That said, in real-world decision-making, “theoretical mechanism” isn’t enough. In review work I’ve done for clients, we focus on what clinical studies actually measured—cognitive endpoints, functional outcomes, and the duration of measurable effects versus symptom fluctuations.
What outcomes people typically seek
Common goals in conversations about Cerebrolysin include:
- Cognitive performance (memory, attention, executive function—depending on the study/indication)
- Neurological function in specific conditions (again, depends on regulatory context)
- Functional recovery where underlying brain injury or neurodegeneration is involved
The key point: outcomes vary by baseline condition, severity, time since onset, and the quality of the clinical protocol (dose, frequency, duration, and concomitant care).
How it’s used in practice (and why that matters for results)
When a therapy is administered under clinical protocols, the variables are controlled in ways that DIY supplement-style decisions can’t match. That’s why the “how” matters as much as the “what.” In my hands-on review experience, I’ve seen people underestimate how strongly protocol differences (treatment schedule, total exposure, patient selection) affect whether an intervention looks effective in studies.
Dihexa vs Cerebrolysin: how to compare them the right way
To compare dihexa vs cerebrolysin responsibly, I recommend you avoid “name-based” comparisons and instead compare by evidence structure and clinical reality.
1) Evidence maturity
- Cerebrolysin: generally discussed with more direct clinical-use framing (where permitted). Outcomes are typically evaluated through controlled studies in defined patient populations.
- Dihexa: often discussed in research hypotheses and narrower evidence contexts. When comparing, you’ll usually see less standardized real-world clinical evidence.
2) Clinical protocol and oversight
- Cerebrolysin is typically handled as a therapy with protocol-driven administration and medical oversight in clinical settings.
- Dihexa discussions frequently land in experimental territory where dosing, purity, and study endpoints may be less standardized across sources.
3) Outcome credibility (what was measured and how consistently)
In evidence-based reviews, I look at:
- Whether endpoints are objective (e.g., validated cognitive scales) or subjective
- Whether effects are sustained or short-lived
- Whether benefits depend on baseline pathology and timing
- Whether results replicate across studies
This is where a “peptide comparison chart” online often fails—because it skips the measurement details. My lesson learned: two interventions with similar “headline mechanisms” can show very different clinical signal strength.
Safety, limitations, and realistic expectations
Any brain-targeting therapy needs a sober safety review. In my work supporting decision-making, I always separate “possible benefits” from “risk and uncertainty.” Peptides and neuroactive agents can differ substantially in tolerability, administration method, and monitoring needs.
Common practical limitations to consider
- Eligibility matters: responses tend to be more variable when starting late (e.g., advanced neurodegeneration) or when comorbidities aren’t addressed.
- Protocol adherence matters: inconsistent timing and insufficient duration can turn “signal” into “noise.”
- Source and quality matter: purity and handling differ widely outside medical channels, which complicates comparisons.
What “effective” realistically means
For brain health, expect outcomes in ranges—improvements in specific domains, stabilization, or slower decline—rather than dramatic reversals for everyone. I’ve guided people who were disappointed because they expected supplement-like “stacking” to produce cognitive transformation. In clinical contexts, the more honest expectation is targeted support within a defined framework.
How to build a decision plan (step-by-step)
If you’re deciding between options discussed under dihexa vs cerebrolysin, use a structured approach:
- Define your goal precisely (e.g., short-term cognitive support vs long-term neuroprotection; memory vs attention vs functional recovery).
- Identify your baseline condition (and time course). Brain interventions behave differently depending on what’s driving symptoms.
- Match intervention evidence to your scenario: prioritize therapies with study endpoints and protocols that resemble your situation.
- Ask about monitoring: what symptoms will be tracked, and what would indicate you should stop or adjust?
- Document outcomes: use the same cognitive/functional measures at consistent intervals so you can tell real change from day-to-day variability.
- Plan for the rest of the brain-health stack: sleep, aerobic activity, vascular risk control, and cognitive training often determine whether any neuro-targeting strategy shows up as “noticeable.”
FAQ
Is dihexa safer than cerebrolysin?
Safety depends on the specific formulation, administration method, and patient profile—not just the peptide name. In practice, Cerebrolysin’s clinical-use framing typically comes with more standardized medical oversight. If you’re considering dihexa, your safety assessment should focus on product quality, dosing protocol, and professional monitoring.
Which one is better for memory and brain health?
“Better” depends on your baseline condition and what studies measured. Cerebrolysin is commonly discussed in more established clinical contexts for neurological indications. Dihexa discussions more often rely on research hypotheses. The most evidence-aligned approach is to choose based on clinical endpoints that match your goal, not on general mechanism claims.
How long until you see results?
In brain health interventions, changes—when they occur—are often gradual and depend on the protocol and the condition being treated. The only dependable way to estimate timing is to look at the treatment duration used in studies relevant to your scenario and track your own outcomes using consistent measures.
Conclusion
When comparing dihexa vs cerebrolysin, the best way to think like a clinician (not a marketer) is to compare evidence maturity, clinical protocol reality, and how outcomes were actually measured. Cerebrolysin is discussed as a neurotrophic-support therapy with more standardized clinical-use framing, while dihexa is more frequently discussed in research-oriented conversations where protocol and endpoint alignment may be less consistent.
Next step: write down your specific brain-health goal and baseline context, then match each option to study endpoints and protocol details from relevant evidence—so your decision is anchored in measurable outcomes, not just peptide names.
Discussion