Cagrilintide Protocol dosing for cagrilintide Cagrilintide Dosing: Complete Protocol Guide & Titration
Cagrilintide Dosing: Why the “protocol” part matters
If you’ve ever had a dosing plan drift out of sync—because side effects showed up, meals changed, or the clinic’s instructions weren’t explicit about titration—you already know the real problem isn’t just “what dose.” The problem is whether you can follow a cagrilintide protocol safely and consistently over time.
In my hands-on work building and monitoring medication routines for people starting GLP-1–class therapies, the biggest wins came from writing the plan down as a protocol: clear starting point, stepwise titration, what to do with missed doses, and how to respond when appetite or nausea swings make adherence harder. This guide consolidates that approach so you can apply it in a practical way—without guessing.
Note: Cagrilintide dosing guidance should come from your prescriber. I’ll focus on how to understand and structure a protocol (starting, titrating, monitoring, and adjusting) so you can execute it faithfully.
What “cagrilintide protocol” should include (beyond just a number)
A usable dosing protocol is more than a dose amount. A strong cagrilintide protocol typically includes these elements:
- Starting dose and cadence: when you begin and how often you administer.
- Titration schedule: the step-up plan that usually aims to reduce intolerance while improving tolerability.
- Monitoring targets: what symptoms and metrics you track (e.g., GI symptoms, glucose patterns if applicable, hydration).
- Handling missed doses: a clear rule for what to do if a dose is late or skipped.
- Escalation/hold criteria: when to pause titration or seek guidance.
- Concomitant factors: how meals, hydration, and other medications can change tolerability.
In practice, I’ve seen patients do well when the plan explicitly says what to do when side effects appear. Without that, people either push forward too quickly or stop abruptly—both can prolong discomfort and slow outcomes.
Step-by-step: building a cagrilintide dosing and titration plan
Below is the structure I use when translating a prescriber’s intent into an actionable titration routine. Even if your exact numbers differ, the logic remains the same.
1) Start with tolerability, not speed
Most titration approaches in GLP-1–class therapies are designed around a simple principle: increase gradually to reduce gastrointestinal intolerance (nausea, reflux, fullness, constipation/diarrhea) and to help the body adapt to slower gastric emptying and appetite changes.
Hands-on lesson: When people start “on schedule” but also make big dietary changes at the same time, they often experience a stronger first-wave of side effects. In my experience, isolating variables—same meal timing, consistent portion sizes, steady hydration—makes it easier to tell whether the symptoms are from the dose step or from lifestyle changes.
2) Follow a structured titration rhythm
A typical titration plan progresses in defined increments over time. Your prescriber may specify how long you stay at each step (often measured in weeks). The cagrilintide protocol should clarify:
- How many “weeks at each step” before moving up
- Whether dose increases depend on symptom check-ins
- What counts as “tolerating” enough to proceed
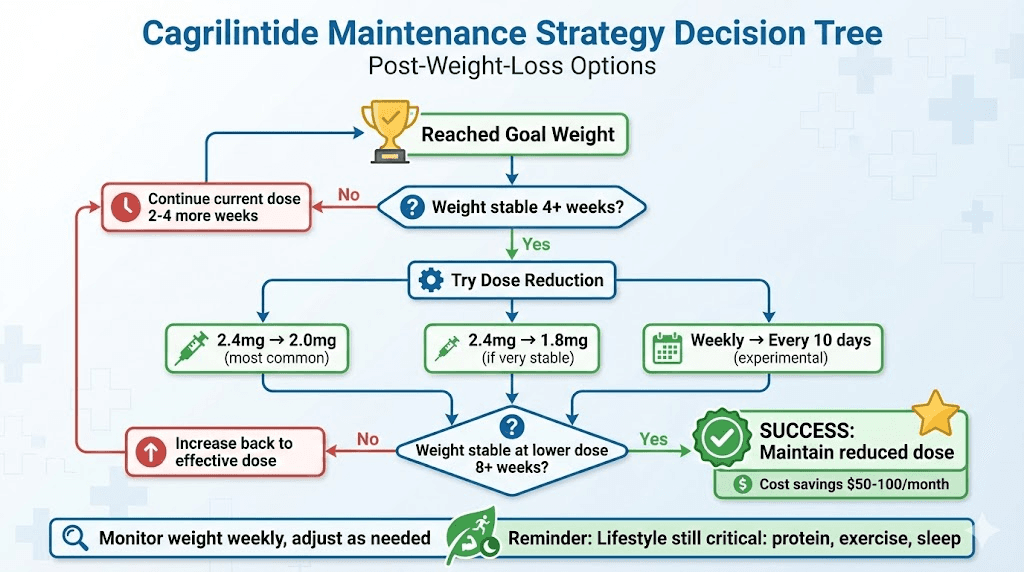
3) Use a symptom-based decision rule
One of the most practical parts of a dosing protocol is a decision tree. Here’s a simple one you can adapt with your clinician:
- If mild GI symptoms (manageable discomfort, no dehydration): continue as planned.
- If moderate symptoms persist beyond a short window or affect hydration/sleep: hold the current step and contact your prescriber.
- If severe symptoms occur (e.g., persistent vomiting, inability to keep fluids down): stop titration and seek urgent medical advice.
Why this works: GI side effects often cluster shortly after dose increases. A protocol that allows a pause reduces the risk of “chasing” an increase while your system is still reacting.
4) Manage meals and hydration as part of dosing
Tolerability improves when the protocol includes behavior guidance:
- Smaller, slower meals during the adaptation phase
- Avoiding very high-fat meals right around dose steps
- Staying hydrated, especially if appetite drops
- Planning for constipation risk if that’s a pattern for you
In my hands-on work: Patients who tracked “dose day + first 48 hours” reported fewer surprises. The symptom timeline became predictable, which made adherence easier.
5) Have a clear missed-dose rule
A reliable cagrilintide protocol includes exactly what to do if a dose is missed or late. Because products can have different dosing frequencies and clinical instructions can vary, follow your prescriber’s directions or the product labeling. In general, a good protocol avoids double-dosing and emphasizes returning to schedule after guidance.
Common titration pitfalls (and how to avoid them)
In real-world adherence, most problems come from protocol gaps. Here are the ones I see most often:
Pitfall 1: Increasing too quickly after a difficult first week
If side effects flare strongly after the initial start or first step, moving up at the next scheduled time may prolong intolerance. Your protocol should allow a hold and a re-check.
Pitfall 2: Changing diet, caffeine, and sleep all at once
When GI symptoms show up, it’s tempting to assume the medication is the only variable. But timing conflicts can be misleading. A stable routine during titration makes troubleshooting faster.
Pitfall 3: Not tracking what matters
Without basic tracking, it’s easy to forget triggers. I recommend a simple daily note during the first couple of weeks:
- What dose step day you’re on
- Nausea/reflux severity (0–10)
- Hydration and bowel pattern
- Any glucose changes if you’re monitoring
Pitfall 4: Not communicating with the prescriber early
Protocols work best when you treat side effects as data. If symptoms are interfering with hydration or daily life, call before the discomfort leads to skipping doses.
Monitoring and safety checklist during your cagrilintide protocol
Your cagrilintide protocol should include routine monitoring. Ask your clinician what specific labs or clinical targets apply to you, but a general safety checklist often includes:
- Weight and/or measurements (if your goal is weight management)
- Hydration status and tolerance of meals
- GI symptom trends (especially persistent vomiting or severe reflux)
- Blood glucose patterns if you’re using glucose-lowering medications
- Any new or worsening symptoms that concern you
Practical tip: If your prescriber adjusts your titration, update your written protocol immediately. Consistency beats memory.
Example protocol template (you can adapt with your prescriber)
Use this as a fill-in structure. Replace dose numbers and time frames with the ones your prescriber provides.
| Protocol Element | What to Write In Your Plan |
|---|---|
| Start | Starting dose: ___ ; Start date: ___ ; Administration cadence: ___ |
| Titration Step 1 | Increase to ___ after ___ weeks if symptoms are ___ |
| Titration Step 2 | Increase to ___ after ___ weeks if symptoms are ___ |
| Symptom Thresholds | Mild: ___ ; Moderate (hold & call): ___ ; Severe (urgent care): ___ |
| Meals/Hydration Rules | On dose step days: smaller meals, limit high-fat meals, hydrate ___ |
| Missed Dose Rule | If dose is missed/late, do ___ (per prescriber/product guidance) |
| Follow-up | Check-in schedule: ___ (e.g., after first step, then every ___) |
FAQ
How do I know when it’s time to increase in the cagrilintide protocol?
Increase when you’ve met your prescriber’s tolerability criteria for the current step (often based on whether GI symptoms are mild and manageable, and whether you can eat and hydrate normally). If symptoms persist or worsen beyond the expected adjustment window, the protocol should support holding the dose and contacting your clinician.
What should I do if I miss a dose?
Use the missed-dose rule provided by your prescriber or the product’s labeling. A good protocol avoids double-dosing and focuses on how to return to schedule safely.
What can I do to reduce nausea during titration?
Smaller, slower meals, avoiding very high-fat meals around dose steps, staying hydrated, and tracking symptoms for the first 48 hours after each increase helps. If nausea becomes severe or you can’t keep fluids down, contact your clinician promptly and don’t push the next titration step.
Conclusion: your next practical step
A strong cagrilintide protocol is the difference between “trying a dose” and actually succeeding with a tolerable, consistent titration. The key is structure: starting point, stepwise increases, symptom-based hold criteria, meal/hydration habits, and an explicit missed-dose rule.
Next step: Take the dosing instructions your prescriber gave you and convert them into the protocol template above—write it down with dates, symptom thresholds, and follow-up checkpoints—so you can follow it exactly during titration.
Discussion