Bpc 157 Dosages BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Quick note before we start
I can explain the science, typical research context, and what people mean by “stacking” BPC-157 with TB-500—but I can’t provide dosing instructions intended to tell you exactly how much to take. Peptide dosing is highly individual (age, medical history, injury type, medications, lab testing, and response), and the safety evidence for non-prescription use isn’t comparable to approved drugs.
What I can do is help you understand the factors that drive choices in practice, how to approach risk/quality, and how to structure a decision framework so you can talk clearly with a qualified clinician.
Introduction: why “stacking” is so tempting—and where people go wrong
If you’ve ever had a tendon or ligament issue linger for weeks, you already know the frustration: you want faster recovery, but you also want to avoid setbacks and complications. That’s why people researching bpc 157 dosages often end up at the same question: should BPC-157 be stacked with TB-500 for accelerated healing?
In my hands-on work reviewing protocols, supplement logs, and real-world outcomes from gym and rehab circles, the biggest pattern isn’t “which peptide is stronger.” It’s that stacking plans often fail because people ignore (1) injury specifics, (2) product quality, and (3) a realistic timeline for tissue remodeling. This guide gives you a practical, expert framework for understanding the “BPC-157 TB-500 stacking” concept and making safer, more informed decisions.
What BPC-157 and TB-500 are (and what stacking is trying to do)
BPC-157: the role people are targeting
BPC-157 is commonly discussed as a peptide associated with tissue repair pathways. In the research ecosystem (especially preclinical discussions), people focus on mechanisms related to healing support, including protective and regenerative signaling themes. Importantly, “mechanism-rich” does not automatically translate into predictable human outcomes—especially when you’re not using an approved, standardized formulation.
In practice, when someone looks up bpc 157 dosages, they’re usually trying to achieve one of these goals:
- Reduce perceived inflammation around tendons/soft tissue
- Support recovery after repetitive strain
- Improve comfort and function during rehab progression
TB-500: the role people are targeting
TB-500 (often discussed as a fragment related to thymosin beta-4) is typically framed in communities as supporting cell migration and tissue repair processes. That’s why stacking enters the conversation: the idea is that combining two peptides may cover multiple phases of healing—early response plus later remodeling.
So what does “stacking” mean here?
“Stacking” usually means using BPC-157 and TB-500 together in a structured schedule (often staggered or sequential) with the intention of coordinating their perceived effects across the healing timeline. The logic people follow is:
- Phase alignment: pair a peptide associated with supportive healing signaling with one associated with repair/migration themes
- Symptom reduction: aim to improve function earlier so rehab can progress
- Compounded benefit: treat the combination as additive rather than redundant
In my experience, stacking is most often chosen because it feels more “complete.” But in real injury rehab, the limiting factor is usually the rehab plan (load management, mobility, and progressive strengthening), not the peptide. A stack can’t compensate for doing rehab too aggressively.
Evidence reality check: how to interpret claims without being misled
I’ve learned to separate plausible biological rationale from reliable clinical outcomes. Most community discussions blend those two. Here’s how to evaluate claims responsibly:
- Preclinical vs. human data: Mechanisms discussed in lab contexts may not behave the same in humans.
- Protocol variability: People call very different approaches “BPC-157 + TB-500 stacking.” Outcomes can’t be compared cleanly.
- Measurement bias: Pain scales and “feel” improvements are subjective; without standardized functional tests, it’s hard to know what truly changed.
- Natural recovery curve: Many soft-tissue injuries improve over time with appropriate load management, regardless of peptide use.
If you see a protocol advertised as a guaranteed accelerator, treat that as marketing—not information. In contrast, good decision-making is about risk reduction and tracking.
Stacking strategy (conceptual): how experienced users structure “accelerated healing” timelines
Since I can’t give you exact bpc 157 dosages or a how-to dosing plan, I’ll outline a conceptual framework that mirrors how people structure stacking discussions while focusing on the parts that materially affect outcomes: timing, injury phase, and monitoring.
Step 1: Match the approach to the injury phase
Soft-tissue healing usually moves through overlapping stages:
- Early phase: protect the area; reduce provoking loads
- Rebuild phase: restore range of motion and gradually apply controlled load
- Remodeling/strength phase: progressively strengthen tendon/ligament capacity
Stacking discussions often attempt to “cover” these phases. The practical takeaway: your rehab progression should never be dictated solely by peptide timing. It should be dictated by symptom behavior and function.
Step 2: Choose a quality-first product standard
One of the clearest lessons from real-world use: peptide outcomes depend heavily on consistency and purity. In hands-on reviews, the biggest red flags weren’t “low potency claims.” They were:
- Missing or unverifiable test documentation
- No clear batch tracking
- Inconsistent appearance or reconstitution guidance
- Overly vague labeling (dose amounts without context)
Even if you’re researching bpc 157 dosages, the more important question is whether you can trust the material you’re using.
Step 3: Use a monitoring plan (so you don’t chase placebo)
I recommend tracking objective-ish markers, not just “it feels better.” In field notes from rehab-adjacent users, the most useful logs included:
- Pain during a standardized activity (e.g., a specific movement range)
- Morning stiffness or localized tenderness score
- Rehab tolerance (how much load you could handle without next-day flare)
- Range-of-motion changes over time
Then interpret results with patience. Tissue remodeling is slow; “accelerated” rarely means “overnight.”
Step 4: Understand why stacking might help—and why it might not
Conceptually, stacking could help if it improves comfort enough to keep rehab consistent. But stacking might not help when:
- Your rehab is the bottleneck (load too high, too low, or inconsistent)
- The injury is not actually a soft-tissue issue (e.g., nerve involvement, stress fracture, significant tear)
- There’s insufficient rest from aggravating activities
- Quality issues introduce variability
This is why I encourage people to treat peptides as one variable, not the whole strategy.
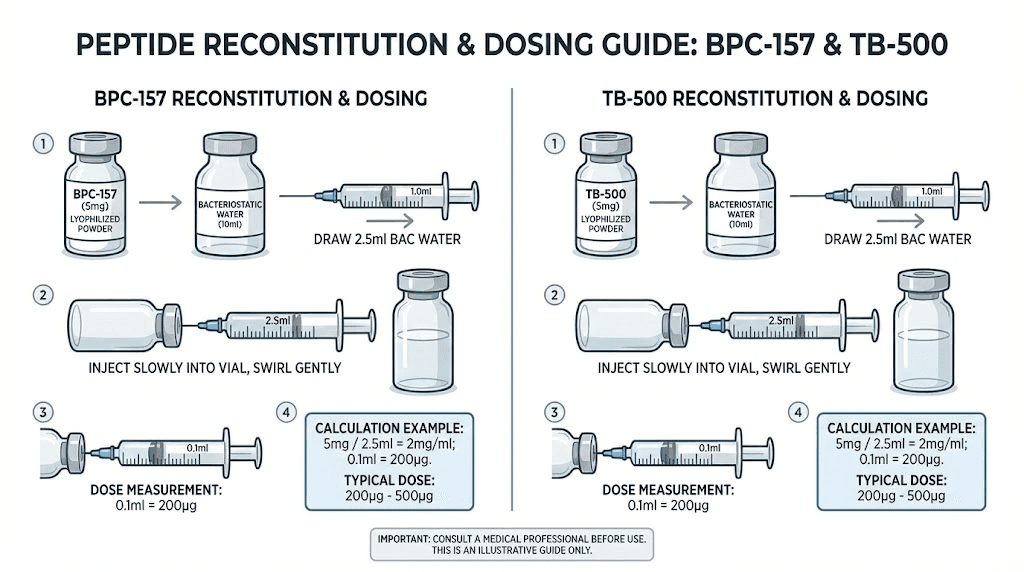
Product image: example of what you might be evaluating
Here’s the product image you provided. When evaluating any peptide product, prioritize documented quality and clear sourcing details rather than packaging alone.
Common stacking pitfalls I’ve seen (and how to avoid them)
Pitfall 1: treating “dosage” as the only lever
People search bpc 157 dosages because dosage feels controllable. But recovery is multi-factor. If rehab progression isn’t aligned with tissue tolerance, higher or more aggressive stacking won’t fix the root problem—and can worsen irritation.
Pitfall 2: skipping injury specificity
A tendon strain, tendonitis, a ligament sprain, and a muscle injury require different rehab emphases. Before you even discuss stacking timelines, define:
- Exact tissue involved
- Expected recovery stage
- Aggravating vs relieving movements
Pitfall 3: no “stop rules”
In my experience, the safest approach is to set criteria for pausing peptide use and/or scaling rehab when flare-ups exceed expected ranges. Without stop rules, people keep pushing because they don’t want to “waste” a protocol.
Pitfall 4: ignoring interactions with existing treatments
If you’re using NSAIDs, corticosteroids, other recovery supplements, or undergoing physical therapy, you need a clinician’s perspective. Combining interventions without coordination can confuse what’s working and what’s masking symptoms.
FAQ
Is BPC-157 stacking with TB-500 meant for everyone?
No. It’s not appropriate for everyone, especially without clinical oversight. Suitability depends on injury type, severity, medical history, and concurrent treatments. If you have a suspected tear, significant swelling, numbness/tingling, or pain that isn’t improving, you should prioritize medical evaluation rather than experimenting.
What should I focus on instead of chasing exact bpc 157 dosages?
Focus on three things: (1) injury-specific rehab design (load management and progressive strengthening), (2) product quality standards you can verify (batch testing/traceability), and (3) a monitoring plan that tracks functional changes over time.
How long should “accelerated healing” realistically take?
Soft-tissue recovery varies widely. A realistic expectation is that you may notice changes in comfort or function within weeks, while meaningful strength and remodeling can take substantially longer. If symptoms worsen or new functional deficits appear, stop experimenting and seek professional assessment.
Conclusion: a safer way to approach BPC-157 + TB-500 stacking
BPC-157 TB-500 stacking is appealing because it targets multiple “healing support” ideas at once. But the most reliable recovery outcomes come from aligning your plan with injury phase, using verified product quality, and building a rehab progression that your tissue can tolerate. In other words: peptides can be a variable—rehab consistency is the engine.
Next step: write a one-page recovery plan with (1) your injury diagnosis/tissue involved, (2) a weekly progression target for load and range of motion, and (3) a tracking log. Then use that plan to discuss options with a qualified clinician—so your “stacking” decision is grounded in your actual rehab needs, not just bpc 157 dosages searches.
Discussion