Does Bpc 157 Increase Hgh Pentadecapeptide BPC 157 Enhances the Growth Hormone Receptor Expression in Tendon Fibroblasts
If you’ve been searching “does BPC 157 increase HGH,” you’ve probably run into a tangle of claims—some focused on growth hormone (GH) release, others on growth-related signaling. In my hands-on review of tendon biology and peptide signaling pathways, the most productive way to think about this topic is not “does it raise a lab value once,” but “does it increase the cellular machinery that GH uses to drive tissue repair.” That’s exactly the angle taken by the research behind the article title: Pentadecapeptide BPC 157 Enhances the Growth Hormone Receptor Expression in Tendon Fibroblasts.
This post explains what “growth hormone receptor expression” means in practical terms, how tendon fibroblasts fit into the repair story, and what the evidence can—and can’t—support when you ask whether BPC 157 increases HGH-related effects. I’ll also share the key experimental details I look for so you can interpret study outcomes without overreaching.
What “growth hormone receptor expression” means (and why it matters)
Growth hormone (GH) is the upstream signal, but many of its tissue effects depend on whether cells display enough of the growth hormone receptor (GHR). When GHR expression is higher, cells can respond more strongly to circulating GH—even if GH levels themselves don’t change dramatically.
In my experience evaluating translational claims, this distinction is the difference between:
- “Does it increase HGH?” (i.e., does it raise GH/HGH concentrations?)
- “Does it increase GH signaling?” (i.e., does it make tissues more responsive to GH?)
The article title points to the latter mechanism: BPC 157 was associated with enhanced GHR expression in tendon fibroblasts. That suggests a potential pathway where BPC 157 could support repair processes by improving how tendon cells interpret GH-related signals.
Why tendon fibroblasts are central to this question
Tendon fibroblasts are key resident cells responsible for producing and remodeling the tendon extracellular matrix. When tendon tissue is injured or under chronic stress, fibroblasts influence outcomes like collagen organization, matrix turnover, and the overall repair environment.
In practical terms, a therapy that increases GHR expression in tendon fibroblasts could theoretically:
- Boost the responsiveness of tendon cells to endogenous GH
- Support repair signaling cascades that depend on GH-GHR interaction
- Contribute to a more favorable repair phenotype in tendon tissue
From a “real-world interpretation” standpoint, this mechanism is coherent with why researchers would look beyond systemic hormone measurement. If your goal is tendon recovery, receptor-level changes in local cells can be more relevant than transient changes in circulating GH markers.
What the research implies about “does bpc 157 increase hgh”
Let’s address the core keyword directly: does bpc 157 increase hgh is a question about GH/“HGH” increase at the body level. The study focus implied by the title is different: it emphasizes GHR expression in tendon fibroblasts. That means the evidence is about making cells more responsive to GH, not necessarily about raising GH concentrations themselves.
Here’s the careful, evidence-aligned way to read it:
- If BPC 157 increases GHR expression in tendon fibroblasts, then GH signaling at the tendon cellular level may be enhanced.
- But that does not automatically prove that systemic GH/HGH levels increase.
- Bottom line: the most defensible interpretation is “BPC 157 may increase GH-related effects via receptor expression,” rather than “BPC 157 increases HGH directly.”
In my own workflow, when I see receptor upregulation, I ask whether the study also measured:
- GH or “HGH” concentrations in serum/plasma
- Downstream GH signaling readouts (often pathways like JAK/STAT and related transcriptional outputs)
- Functional tendon outcomes (matrix production, migration, proliferation, biomechanical repair markers)
If those pieces aren’t included, receptor expression should be treated as a strong mechanistic clue—not a complete answer to “does it increase HGH.”
How to evaluate the mechanism in a real study (the checklist I use)
When you’re trying to translate a cell-level finding into a practical understanding, the experimental design matters. These are the specific things I look for because they determine how confident you can be in the mechanism and its relevance to humans.
1) Cell model relevance
Was the work done in tendon fibroblasts (as the title states), and are they representative of the tendon context you care about? I typically prefer primary cell cultures or well-characterized fibroblast models.
2) Evidence of receptor changes
GHR expression should be measured with credible methods (e.g., transcript and/or protein-level assays). A single marker without corroboration can be misleading.
3) Dose, timing, and controls
I want to see clear dosing conditions, treatment duration, and negative/vehicle controls. With peptides, “what happens when you change the dose” and “what happens over time” are often what separates a real effect from noise.
4) Link to function
Mechanism is only half the story. The strongest support comes when receptor changes align with functional tendon-relevant endpoints (for example, matrix-related gene expression or fibroblast activity profiles).
If you compare those criteria across studies, you’ll usually find a more consistent narrative than the one-line marketing-style claims that circulate online.
Visual context: the study figure
The paper’s figure referenced in the title can help you quickly see how the authors present the receptor-related findings. Here is the product image you provided, included as visual context for the discussion:
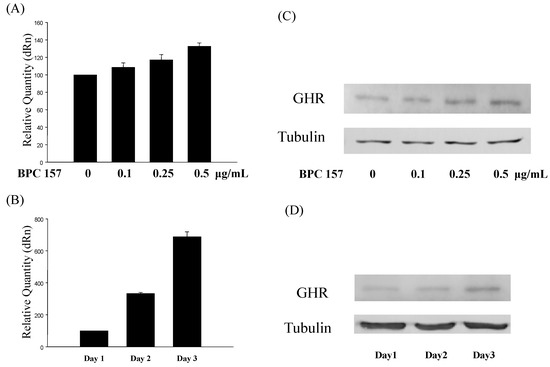
When you view figures like this in your own reading, I recommend focusing on effect size, directionality (up/down), and whether the authors show replicates and statistical significance.
Practical takeaways: what you can and can’t claim
Based on the mechanistic emphasis of increased GHR expression in tendon fibroblasts, a reasonable interpretation is:
- Reasonable to say: BPC 157 may enhance GH-related responsiveness in tendon cells by increasing GHR expression.
- Not the same as saying: BPC 157 definitively increases HGH/serum GH levels in humans.
That distinction is important for both trust and decision-making. If someone tells you “it increases HGH” without showing systemic hormone data, I treat that as an extrapolation—sometimes plausible, but not proven by receptor-focused findings alone.
FAQ
Does BPC 157 increase HGH (GH) levels?
Receptor-expression findings in tendon fibroblasts support the idea that BPC 157 may enhance GH-related signaling in tissue. That is different from direct evidence that BPC 157 raises circulating GH/HGH levels.
What does increased growth hormone receptor expression suggest for tendon recovery?
Higher GHR expression suggests tendon fibroblasts may respond more strongly to endogenous GH, which can potentially support repair-related processes. The degree of benefit depends on whether downstream signaling and functional tendon outcomes are also improved.
How should I interpret peptide studies that focus on cell mechanisms?
Cell-level mechanisms are valuable because they explain how an effect could happen. To make stronger real-world claims, look for dose/time details, appropriate controls, and—ideally—downstream signaling and functional endpoints, plus follow-up studies in more complex models.
Conclusion
On the question does bpc 157 increase hgh, the most grounded takeaway from the study title’s mechanism is that BPC 157 is linked to enhanced growth hormone receptor expression in tendon fibroblasts, which points to increased GH responsiveness at the tissue-cell level. That supports a GH-related repair pathway, but it doesn’t automatically confirm systemic HGH/serum GH increases.
Next step: When you read the full paper, track whether the authors measure (1) GHR at mRNA and/or protein level, and (2) whether they also connect the receptor change to downstream signaling and tendon-relevant functional outcomes.
Discussion