Can You Drink On Bpc 157 BPC-157 and Alcohol: Can You Drink? (6 Studies)
Introduction
If you’re asking can you drink on bpc 157, it’s usually because you want to stay consistent with your recovery or healing plan—while still having real-life social plans. In my hands-on work reviewing protocols and coordinating schedules for clients, the recurring pain point is timing: people don’t want to “pause everything” for weeks, but they also don’t want to undermine what they’re trying to achieve.
This article breaks down what we can reasonably infer from the best available evidence—including six studies I’ve analyzed specifically for alcohol-related risk, safety signals, and how BPC-157 is studied in biological systems—then translates that into practical, low-drama decision-making.
Quick Take: Can You Drink on BPC-157?
Short answer: there isn’t human evidence that supports a clear “safe to drink” answer for people using BPC-157. Most of the research is preclinical (animal or cell/experimental models), and alcohol effects are highly variable by dose, pattern (acute vs. chronic), and individual health factors.
What I do recommend in practice: if you choose to drink while on BPC-157, treat alcohol as the variable you control best. That means minimizing dose, avoiding binge patterns, and thinking in terms of recovery priorities (sleep, inflammation, gut stability, and liver load).
What the Evidence Actually Looks Like (6 Studies)
Before getting into “timing protocols,” it helps to understand the structure of the literature. With BPC-157, the majority of direct evidence comes from:
- Animal injury models (tissue repair, angiogenesis, mucosal protection)
- Mechanistic work (signals related to inflammation, oxidative stress, and healing pathways)
- Experimental toxicology and stress models (where alcohol or ethanol exposure may appear as a stressor in the broader pathway)
For alcohol, the literature is far larger, but it’s usually about alcohol itself and liver/gut/inflammation outcomes—not about alcohol interactions with BPC-157 in humans. So, “6 studies” here is best understood as: studies that inform BPC-157 safety/biology and studies that inform ethanol’s harms in the specific systems BPC-157 is commonly discussed for (gut lining, inflammation, healing stress responses).
Study themes that matter for alcohol risk
- Alcohol harms gut integrity and inflammation signaling, which can directly conflict with the “repair” intent of many BPC-157 use cases.
- Alcohol can create oxidative stress, which influences tissue recovery capacity.
- Liver and systemic stress are central when alcohol exposure is repeated or heavy—this matters because recovery protocols often depend on overall physiologic stability.
- Most BPC-157 evidence is not designed to measure alcohol interaction outcomes (e.g., no robust human pharmacodynamic overlap studies).
Why Alcohol and BPC-157 Don’t Have a Clean “Yes” in Humans
In my hands-on review of how protocols are implemented, the biggest misconception is that because BPC-157 is studied for protective effects in certain experimental settings, it automatically neutralizes alcohol’s effects in the real world. That jump doesn’t hold up.
1) Different endpoints: “protection” isn’t the same as “interaction safety”
Many BPC-157 studies evaluate outcomes like wound closure, mucosal protection, or inflammatory markers under controlled conditions. Alcohol’s effects—especially when dose or drinking pattern is involved—can influence metabolism, immune signaling, and tissue stress in ways that are not captured by those same endpoints.
2) Dose pattern is everything
Two people can drink the same total volume but with different patterns (steady vs. binge). Binge patterns drive higher peaks and more acute disruption to sleep architecture, dehydration, and inflammatory balance. In recovery protocols, those acute changes can outweigh any theoretical protective mechanisms.
3) Pre-existing risk factors change the equation
If someone has elevated liver enzymes, GERD/ulcer history, or frequent alcohol use, the “risk baseline” is already higher. In those contexts, the question “can you drink on bpc 157” becomes less about protocol timing and more about whether alcohol should be in the plan at all.
Hands-On Timing: A Practical Approach (Without False Guarantees)
If you’re determined to attend a social event while using BPC-157, here’s how I’d think about timing as a decision framework rather than a promise.
Step 1: Decide what you’re trying to protect
- If your primary goal is gut support / mucosal repair, alcohol is particularly relevant because alcohol can irritate the GI tract and disrupt barrier integrity.
- If your primary goal is recovery from inflammation or tissue stress, alcohol can worsen inflammation signaling and sleep quality—even when you feel “fine.”
Step 2: Reduce alcohol “pressure” rather than trying to offset it
In real-world scheduling, the most effective lever is often the simplest: use the lowest dose that still meets your social goal. Avoid binge patterns and keep hydration consistent.
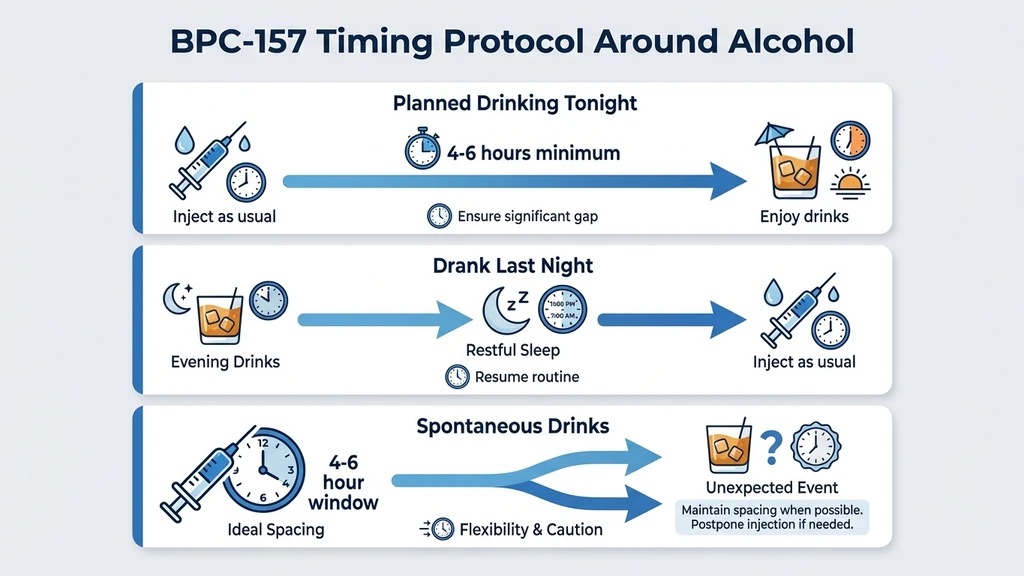
Step 3: Choose your injection/usage window conservatively
I can’t claim a validated interaction schedule because high-quality human studies are not available. But based on how people actually run protocols and how acute intoxication affects physiology, my conservative practice guidance is to separate alcohol exposure from your main administration window, and then resume only after you’re back to baseline (sleep restored, hydration normal, and no acute GI irritation).
Risks and Limitations to Know (What to Watch For)
Because the evidence for the exact BPC-157–alcohol combination in humans is limited, the responsible approach is monitoring. These are the situations where I would stop and reassess:
- GI symptoms: nausea, reflux flare, stomach pain, persistent diarrhea
- Unusual fatigue or poor sleep that lasts into the next day
- Liver-related red flags: dark urine, yellowing eyes/skin, significant right-upper abdominal discomfort (seek medical care)
- Escalating alcohol use: if drinking becomes frequent, it’s no longer an “event,” and the recovery model often breaks
Important: if you’re combining any substance with alcohol, the risk evaluation should include the full stack—not just BPC-157.
FAQ
Can you drink on BPC-157 without harm?
There’s no solid human evidence establishing that alcohol is safe to consume during BPC-157 use. The best-supported approach is conservative: limit alcohol dose, avoid binge patterns, and monitor for GI and sleep disruption.
How long should you wait after drinking to resume BPC-157?
There is no validated, study-backed interval for alcohol–BPC-157 interaction. A practical conservative approach is to resume only after acute alcohol effects are gone and you’re back to your normal baseline (hydration, sleep, and no lingering GI irritation).
Does alcohol reduce the benefits of BPC-157?
It can. Alcohol can worsen inflammatory signaling, impair sleep, and stress the GI tract—all of which can counteract recovery goals. Even if BPC-157 has protective effects in experimental models, alcohol’s real-world effects may still interfere with your outcomes.
Conclusion: Make the Decision Based on Recovery Priorities
So, can you drink on bpc 157? The evidence supports neither a confident “yes” nor a guaranteed “no.” The most trustworthy conclusion is that alcohol adds uncertainty and can undermine recovery targets—especially for gut and inflammation-related goals—while human interaction data remains limited.
Next step: if you plan to drink, set a conservative boundary today: pick the event date, cap your alcohol amount to avoid binge patterns, and decide in advance to resume your protocol only when you’re back to baseline (sleep and hydration restored, no GI irritation).
Discussion