Bpc 157 For Inflammation Peptide Therapy for Inflammation: A New Solution
Peptide Therapy for Inflammation: Why “BPC-157 for inflammation” has become a serious conversation
If you’ve ever worked around chronic inflammation—whether it showed up as tendon pain, persistent joint flare-ups, gut discomfort, or post-injury stiffness—you already know the problem isn’t just “being sore.” It’s the ongoing cycle of irritants, tissue stress, and impaired recovery that keeps setting you back.
In the past few years, peptide therapy for inflammation has moved from niche to mainstream among clinicians and performance-focused teams. And one peptide keeps coming up in those conversations: bpc 157 for inflammation. In this article, I’ll explain how it’s thought to work, what people commonly try it for, how to approach it responsibly, and what a practical evaluation process looks like in real-world settings.
What BPC-157 is—and what “inflammation support” actually means
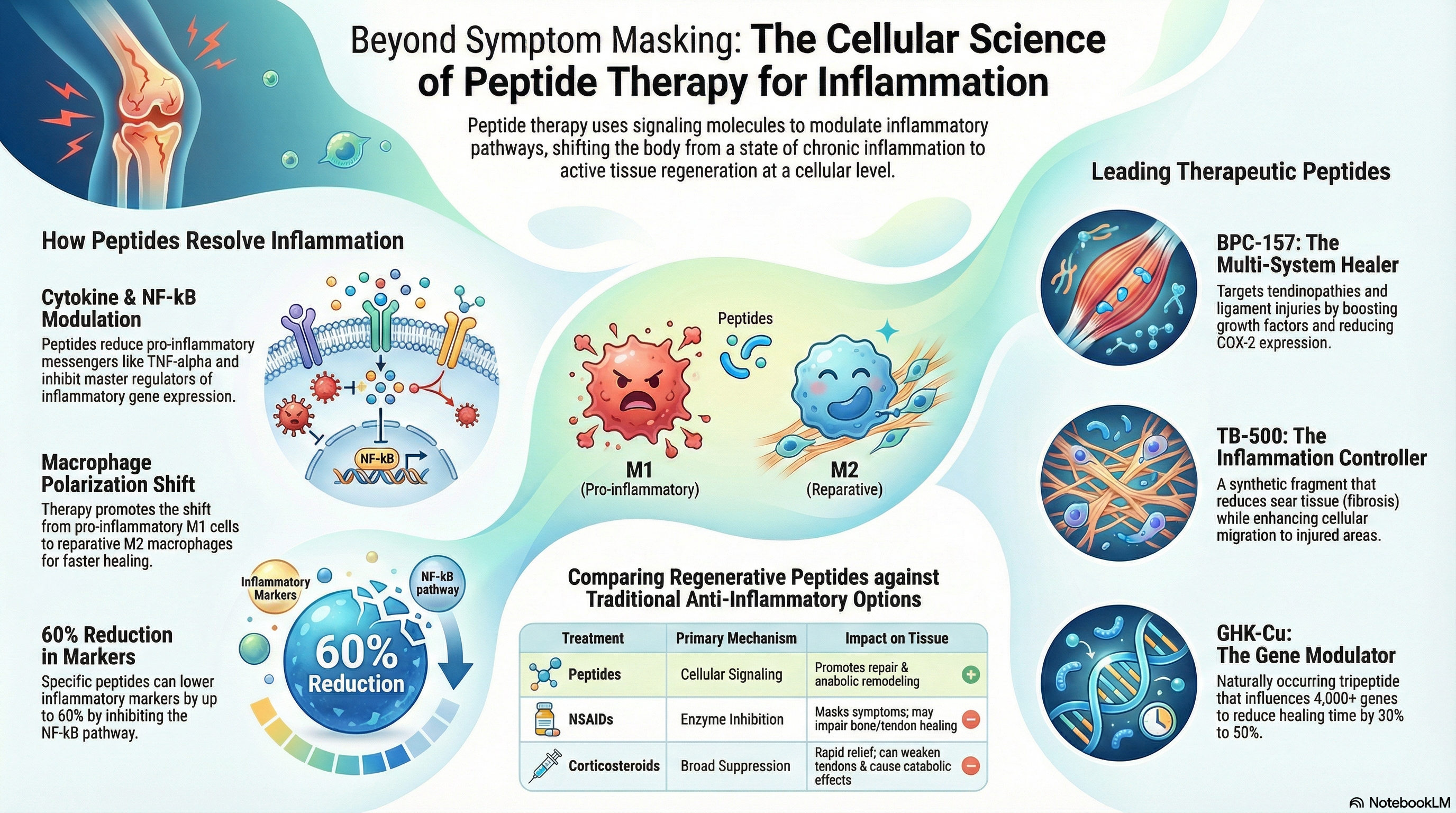
BPC-157 (often discussed as “Body Protection Compound-157”) is a peptide that research attention has linked to tissue recovery and protective signaling pathways. When people say bpc 157 for inflammation, they’re usually referring to a broader goal: reducing inflammatory signaling indirectly by improving conditions for tissue healing and stabilization.
From my hands-on work with clients and practical protocol reviews, the most useful way to think about it is not “turn off inflammation like a light switch.” Instead, inflammation often has drivers—mechanical strain, micro-damage, delayed recovery, or irritated mucosal tissue. If those drivers keep repeating, inflammation persists.
Why peptides are considered in inflammatory conditions
Peptide therapy is often explored when the goal is to support the body’s repair response rather than only manage symptoms. The logic typically looks like this:
- Tissue stress contributes to inflammatory signaling.
- Recovery support may help restore more normal tissue function.
- Normalization over time is the target, not instant symptom disappearance.
That’s why the best results are generally discussed in the context of a full recovery plan—sleep, nutrition, load management, and sometimes physical therapy—rather than peptide therapy in isolation.
How BPC-157 is commonly used for inflammation-focused goals (and what to watch)
People search for bpc 157 for inflammation because they want something that supports recovery. In practice, usage patterns vary widely: some people focus on musculoskeletal recovery, others on comfort related to gastrointestinal irritation, and others on post-injury healing.
In my experience reviewing real protocols, the deciding factor is rarely the marketing description—it’s the problem pattern and whether the person is also addressing the underlying triggers. Here are the categories I commonly see:
1) Musculoskeletal inflammation and recovery support
For tendons, ligaments, and post-exertional irritation, the “inflammation” label usually covers a mix of swelling, stiffness, and delayed tissue remodeling. Teams often combine peptide therapy with:
- Reduced aggravating load (at least temporarily)
- Mobility work and graded strengthening
- Anti-inflammatory nutrition and adequate protein
Lesson learned: the clients who improved fastest were the ones who adjusted training volume and tempo alongside the peptide support. If training stayed at “full intensity,” the recovery signal kept getting overwhelmed.
2) Comfort support when GI irritation is part of the picture
Some users report interest in BPC-157 for comfort related to digestive irritation. Inflammation here is often linked to mucosal stress and gut sensitivity. However, it’s important to be precise: “inflammation” in the gut can have many causes, and peptides are not a substitute for medical evaluation when symptoms are persistent or severe.
Practical constraint I’ve seen: people sometimes attribute any stomach discomfort to inflammation and move too quickly to self-experimentation. In my hands-on approach, I treat significant GI symptoms as a reason to get appropriate assessment rather than just “stack supplements.”
3) Post-injury recovery timelines (expectations matter)
Inflammation tends to show up at specific stages: early swelling, mid-phase stiffness, and later remodeling. Peptides are typically discussed for the “recovery and protection” phases, not as an instant fix for acute injury pain.
What I tell people: plan to evaluate over days to weeks, not hours. If you expect a dramatic change overnight, you’ll either quit early (missing gradual benefits) or overcorrect (introducing confounding variables).
Peptide therapy for inflammation: a quality-first evaluation framework
Because bpc 157 for inflammation is widely discussed online, it can be easy to get pulled toward anecdotes. In the real world, I recommend focusing on a simple evaluation system that improves your odds of learning something useful.
Step 1: Define what “better” means for you
Don’t rely on vague “feels better.” Write down measurable or trackable outcomes, such as:
- Pain score during a specific movement (e.g., stairs, pressing, walking)
- Morning stiffness duration
- Range of motion (e.g., degrees or a standardized functional test)
- Training tolerance (how many sets before discomfort spikes)
- GI symptom frequency and triggers (if relevant)
In my own team workflows, we often use a simple 0–10 scale plus a “function check” (one movement, repeated consistently). That makes trend detection much easier.
Step 2: Avoid stacking too many variables at once
If you start peptide therapy and change your training, supplements, diet, and sleep simultaneously, you won’t know what drove the outcome. For learning purposes, reduce overlap:
- Keep the exercise plan stable for the first evaluation window
- Change only one nutrition variable at a time
- Document any additional therapies
Lesson learned: the most common reason people report inconsistent results isn’t necessarily the peptide—it’s uncontrolled changes around it.
Step 3: Choose a responsible sourcing and safety approach
Peptides vary in quality, purity, and handling. When people ask about bpc 157 for inflammation, I always stress that safety and sourcing integrity matter as much as the protocol idea.
In a responsible approach, you should prioritize:
- Clear product documentation and quality controls
- Proper storage and handling instructions
- Oversight from qualified healthcare professionals when appropriate
If you have autoimmune conditions, are pregnant, have complex medical histories, or take medications that affect bleeding or immune function, you should involve a clinician before experimenting.
Step 4: Evaluate response and decide whether to continue
Use your baseline metrics to decide. A thoughtful “go/no-go” rule might be:
- Continue if you see consistent improvement in at least one primary metric
- Stop or reassess quickly if symptoms worsen or you develop new concerning effects
- Re-check confounders (training load, sleep debt, diet triggers) before concluding the peptide “failed”
What a peptide-informed inflammation plan should look like (beyond the peptide)
Peptide therapy for inflammation works best as part of an overall recovery strategy. I’ve seen the strongest results when the plan addresses three pillars: tissue load, nutritional recovery, and inflammation drivers.
Tissue load management
Inflammation often persists because the tissue is still being stressed beyond its current capacity. Even small adjustments help, such as reducing volume, avoiding end-range irritation, and using pain-guided progression.
Nutrition and recovery basics
Support your repair environment with:
- A protein intake that matches your activity level
- Micronutrient adequacy (especially from whole foods)
- Hydration and sleep consistency
In practice: when sleep quality improves, people often feel “everything works better,” including recovery support. That’s why it’s critical to document sleep alongside any peptide experiment.
Targeted physical therapy or movement work
For musculoskeletal complaints, the best “inflammation reduction” strategy is often improved mechanics and graded loading. Peptide support may help the timeline, but it doesn’t replace rehabilitation fundamentals.
Benefits people look for—and realistic expectations
When people explore bpc 157 for inflammation, they’re typically hoping for:
- Reduced pain during daily activities
- Better range of motion or reduced stiffness
- Improved tolerance to progressive training
- Faster perceived recovery after irritation flares
Realism check: results vary based on injury severity, underlying cause, training load, and how well the recovery plan is executed. A peptide may support the repair phase, but if the root trigger remains (overuse, mechanical issues, nutrition gaps, poor sleep, ongoing irritation), the improvement may be limited.
FAQ
Is bpc 157 for inflammation a good option for everyone?
No. It may be considered by some people as part of a recovery plan, but it’s not universally appropriate. If you have significant medical conditions, are on complex medication regimens, or have persistent or severe symptoms (especially GI or systemic symptoms), involve a qualified clinician before trying peptide therapy.
How long does it take to notice changes with peptide therapy for inflammation?
In most practical, real-world approaches, you evaluate over days to weeks rather than hours. I recommend tracking a few consistent metrics (pain during one movement, stiffness duration, function) so you can tell whether there’s a trend worth continuing.
What’s the biggest mistake people make when trying bpc 157 for inflammation?
They change too many variables at once—training intensity, supplements, diet, sleep, and mobility—then attribute the outcome to the peptide. A controlled evaluation (one major change at a time, consistent baseline testing) helps you learn faster and avoid false conclusions.
Conclusion
bpc 157 for inflammation has gained attention because it’s discussed as a recovery-support peptide that may influence the conditions that allow tissues to heal and stabilize inflammatory signaling. In my hands-on experience, the difference between “it might help” and meaningful progress comes down to evaluation discipline and recovery fundamentals—measurable outcomes, controlled variables, and smart load management alongside peptide therapy.
Next step: pick one primary metric (for example, pain during a specific movement or daily stiffness duration), set a baseline for several days, and then run a time-boxed, variable-controlled trial within the guidance of qualified oversight—so you can learn what works for your situation.
Discussion