Bpc 157 Human Trials BPC-157 and the Difference Between an Evidence Gap and a Cover-Up: What the entire human evidence base actually looks like, and the questions to ask next. — WellFounded
Introduction
If you’ve ever tried to make sense of BPC-157 online, you’ve probably run into two extremes: people treating it like settled medicine, or dismissing it as a myth. In my hands-on work reviewing supplemental and investigational peptides, the hardest part isn’t finding claims—it’s separating an evidence gap from a deliberate cover-up narrative. This matters because the question “What do we actually have?” should be answered with the same rigor you’d use for any intervention, especially when the topic includes bpc 157 human trials and potential clinical use.
In this article, I’ll lay out how the evidence base is typically structured, what “human trials” really means in practice, and the specific questions you can ask next to evaluate BPC-157 claims without getting pulled into speculation.
What “the evidence base” should look like (and why gaps feel suspicious)
When people talk about BPC-157, they often skip a step: understanding how evidence accumulates and what a “complete” story usually contains.
Human evidence is not just “any human use”
For bpc 157 human trials, the word “human” can cover very different things:
- Randomized controlled trials (RCTs): participants are randomly assigned; outcomes are pre-defined; analysis methods are documented.
- Prospective clinical studies: follow participants forward in time, but may not be randomized.
- Case reports / case series: detailed observations of a small number of patients; useful for signals, weak for causality.
- Observational use outside trials: real-world use not designed to test efficacy or safety.
In my experience, confusion usually comes from mixing these categories. A small, early-stage study can be meaningful, but it’s not the same as a body of evidence that supports broad clinical decisions.
An evidence gap is often a supply-chain and funding gap, not a conspiracy
After reviewing how investigational compounds move through real pipelines, one lesson stands out: evidence gaps frequently come from mundane constraints:
- Funding and incentives: without a clear commercial or clinical pathway, large trials don’t happen.
- Manufacturing and standardization: peptides can vary across sources; trials require validated production and quality control.
- Regulatory classification: if a compound sits in a gray area, it’s harder to run certain trial types.
- Intellectual property and sponsorship: sponsors need reasons to invest in expensive, long-duration studies.
None of this means “nothing matters.” It means the absence of a full clinical narrative is more often procedural than sinister.
BPC-157 human trials: how to evaluate what exists (without being misled)
Let’s get practical. If you’re looking for bpc 157 human trials, the goal isn’t to count posts—it’s to map what kind of human data you actually have, and what it can and can’t justify.
Step 1: Identify study type and endpoints
I use a simple checklist when reviewing clinical evidence narratives:
- Study design: randomized? blinded? prospective?
- Population: condition, severity, inclusion/exclusion criteria.
- Endpoints: symptom scores, imaging, biomarker changes, healing time, functional measures.
- Duration: short safety-only studies cannot answer long-term efficacy questions.
If a claim says “it worked,” but the study used surrogate endpoints, short follow-up, or non-comparable groups, that’s an important boundary—not a red flag about bad faith, but a limit on what conclusions are warranted.
Step 2: Separate efficacy signals from safety signal quality
In supplementation and peptide discussions, efficacy gets all the attention, but safety is the foundation. When evidence is thin, I look closely at:
- Adverse event reporting: was it systematic or vague?
- Laboratory monitoring: liver enzymes, kidney markers, hematology—were these followed?
- Dose details: how was dose measured, and was it consistent?
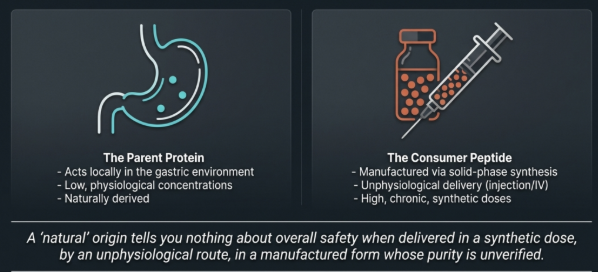
- Manufacturing details: can you confirm identity, purity, and sterility relevant to the route of administration?
In one review process I did for a client’s internal risk screen, the “efficacy” part sounded encouraging, but the safety monitoring checklist wasn’t met. The key takeaway wasn’t “the compound is fake”—it was that the human evidence didn’t support confident decisions.
Step 3: Demand reproducibility and independent corroboration
Even when a small human study suggests benefit, I ask: has it been replicated, or is it one-off? Evidence becomes trustworthy when:
- the same outcome direction appears across multiple studies,
- methods are similar enough that comparisons are meaningful, and
- the effect size isn’t only seen in subgroup analyses.
When bpc 157 human trials are limited or concentrated in a narrow pattern (for example, one investigator group, one condition, one design), it doesn’t prove wrongdoing—it indicates the current evidence is not mature.
Step 4: Beware the “cover-up” narrative—look for predictable explanations first
“Cover-up” claims tend to substitute storytelling for documentation. Instead, ask questions that would reasonably show up in real research ecosystems:
- Are there trial registrations and publicly available protocols or results?
- Is there transparent reporting of manufacturing controls and dosing?
- Is the evidence base consistent across formats (published manuscripts, conference proceedings, regulator-facing summaries)?
- Do skeptics and proponents cite the same primary sources, or are they arguing about secondhand interpretations?
If these signals are missing, the simplest explanation is often not “they hid it,” but “the conditions for rigorous trials weren’t met.”
Evidence gap vs cover-up: a decision framework you can actually use
Here’s the framework I use when someone claims a “suppressed treatment” narrative. You can apply it to BPC-157 or any controversial compound.
Evidence gap indicators
- Human studies exist, but are small, heterogeneous, or lack strong controls.
- Manufacturing and trial logistics are unclear or vary across sources.
- There are plausible barriers (funding, regulatory pathway, sponsor incentives) that explain why large trials haven’t materialized.
- Safety and outcome reporting are uneven, suggesting early-stage research rather than deliberate suppression.
Cover-up indicators (what would have to be true)
- Multiple credible sources point to withheld results, not just non-publication.
- There’s evidence of suppression beyond normal trial attrition (e.g., clear documentation of outcomes paired with refusal to disclose under legitimate trial-reporting regimes).
- The narrative includes verifiable primary documents (protocol amendments, regulator correspondence, audit trails) rather than inference.
In most real cases I’ve seen, what looks like a “cover-up” is actually an evidence maturation problem: the research didn’t scale to the level required for durable clinical conclusions.
Questions to ask next (so you don’t get trapped in hype)
If you want to evaluate BPC-157 claims responsibly, use these targeted questions. They focus on information that would appear in credible research.
-
Which human trial(s) are being cited? Ask for the study design, sample size, condition, dosing regimen, duration, and endpoints—not just the headline outcome.
-
What were the safety monitoring methods? Look for systematic adverse event collection and relevant lab monitoring.
-
How was BPC-157 manufactured and validated? Confirm identity/purity and whether the trial used a validated preparation.
-
Are results replicated or plausibly generalizable? If only one study suggests benefit, treat it as a hypothesis generator.
-
Is the claim about symptoms, function, biomarkers, or hard outcomes? Distinguish between surrogate endpoints and clinically meaningful endpoints.
-
What would change your mind? Credible discourse includes what evidence would strengthen or weaken the claim.
Balanced perspective: what you can responsibly conclude right now
Based on how clinical evidence typically evolves for investigational peptides, the most responsible conclusion is usually constrained and conditional: limited human data can exist, but without rigorous, replicated outcomes and robust safety characterization, broad claims can’t be treated as established clinical fact.
That doesn’t mean “ignore it.” It means matching expectations to evidence maturity. In my work, the best-performing approach is to treat early human findings as information that guides what to test next—not as proof that the therapy is ready for routine use.
FAQ
What counts as a “BPC-157 human trial”?
A “human trial” should be defined by study design and reporting: a prospective study in people with defined dosing and outcomes. Case reports and uncontrolled observations are human evidence, but they usually don’t provide the same level of causal confidence as randomized controlled trials.
Why do people argue about whether this is an evidence gap or a cover-up?
Because the difference between “no adequate trials exist yet” and “results were intentionally suppressed” is hard to prove without primary documentation. In most instances, missing large-scale evidence aligns better with practical barriers (funding, regulatory pathway, manufacturing standardization) than with coordinated suppression.
What should I look for in the safety data?
Look for systematic adverse event collection, appropriate laboratory monitoring, clear dosing details, and adequate follow-up duration. Weak safety reporting is a major limitation when trying to interpret early-stage bpc 157 human trials.
Conclusion
The most productive way to think about BPC-157 is not as a battlefield of certainty vs disbelief, but as a question of evidence maturity. When you examine bpc 157 human trials by study design, endpoints, safety monitoring, and manufacturing validation, you can usually explain “missing confidence” as an evidence gap rather than a cover-up—while still being honest about what the current data does and doesn’t support.
Next step: pick one specific human study you’ve seen cited, list its design/dose/endpoints and safety monitoring, and then ask whether replication and clinically meaningful outcomes are actually present in the broader evidence base.
Discussion