Bpc 157 Adverse Effects Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
If you’re researching BPC-157, one of the first things I see people ask in my inbox and in lab/clinical forums is “What are the bpc 157 adverse effects?” That question matters because peptide research often moves faster than the public safety data. In this article, I’ll break down what the literature and patents say about BPC-157’s multifunctionality and where potential medical applications may fit—while staying grounded in what’s actually evidenced.
I’ll also explain how to interpret adverse-effect information correctly (including the limits of animal-only data), and I’ll highlight the practical lessons I’ve learned when reviewing pharmacology papers and patent claims for translational credibility.
What BPC-157 Is (and Why Multifunctionality Keeps Coming Up)
BPC-157 is a peptide often discussed for tissue-protective and healing-related effects. In many reviews, it’s described as “multifunctional” because researchers report activity across multiple biological endpoints—examples frequently discussed include gastrointestinal protection, modulation of inflammation, effects related to angiogenesis, and impacts on tissue repair signaling.
In my hands-on literature reviews, I’ve found that “multifunctionality” can mean two different things:
- Broad pharmacology: the peptide seems to influence multiple pathways in preclinical systems.
- Broad experimental outcomes: different studies measure different endpoints (ulcer area, inflammation markers, collagen remodeling, etc.), so the overall picture looks wide.
Both interpretations can be true. But for translational decisions, it’s not enough to list endpoints—you have to ask whether the studies share a consistent mechanism or whether they’re simply associating the peptide with improvements in each separate model.
How I Review Claims of Medical Application (Literature vs. Patent)
Patents can be valuable because they often consolidate technical details and intended therapeutic targets. However, patent language is not the same as clinical evidence. To keep my reviews rigorous, I typically separate:
- Evidence type: peer-reviewed studies (methods, endpoints, statistics) versus patent claims (scope, novelty, intended use).
- Strength of outcome: statistically meaningful effect sizes, dose-response clarity, and reproducibility.
- Safety signals: not just “no obvious problems,” but systematic adverse-effect monitoring (e.g., body weight, organ histology, hematology/chemistry panels, behavioral changes).
This is where bpc 157 adverse effects questions deserve careful framing. Many discussions online focus on whether “side effects exist,” but the better question is: in what models, at what doses, and with what monitoring? In preclinical work, “no major adverse effects” can still hide mild toxicity, transient changes, or endpoints that weren’t measured at all.
Multifunctionality in the Evidence: What the Research Commonly Targets
Across the body of work frequently cited around BPC-157, there is a recurring theme: the peptide is investigated as a protective or restorative agent. The medical application areas discussed most often fall into a few buckets. I’ll summarize them at a “decision-useful” level—what the claimed effects aim to accomplish and why that matters for safety interpretation.
1) Gastrointestinal and mucosal protection
GI protection is one of the most prominent contexts in which BPC-157 is discussed. If a compound influences mucosal integrity and inflammatory signaling, it can show benefit in ulcer models or inflammation-associated GI injury.
Safety angle for bpc 157 adverse effects: GI-protection studies sometimes fail to capture systemic toxicity comprehensively. When the study design is narrowly focused on local tissue endpoints, you may not see subtle systemic adverse signals. That’s why broad safety profiling matters more than “it helped the lesion.”
2) Tissue repair and wound-healing pathways
Another major theme is wound healing—often described via improvements in tissue remodeling, histological quality, and markers linked to repair processes.
Safety angle: tissue repair activity sounds “naturally beneficial,” but pathway modulation can theoretically have off-target consequences (for example, effects on unwanted growth signaling). Whether that happens is an empirical question, and good studies should include more than local healing scores.
3) Inflammation modulation
Inflammation is frequently addressed because reducing inflammatory cascades can indirectly improve healing outcomes in multiple tissues.
Safety angle: immunomodulation can be a double-edged sword. The “adverse effects” question should include whether immune function, infection susceptibility, or prolonged inflammatory suppression were monitored—often not fully assessed in early-stage studies.
4) Vascular and angiogenesis-related signals
Some research frames BPC-157 within vascular repair or angiogenesis-related mechanisms, which is part of why multifunctionality is emphasized.
Safety angle: angiogenesis is a tightly regulated process. In translational research, one key question is whether the compound’s vascular effects are controlled, transient, and context-specific—or whether they produce dysregulated remodeling. Patent claims may reference these concepts, but only systematic safety studies can confirm risk.
What About BPC-157 Adverse Effects? (How to Interpret What You Find)
When people search “bpc 157 adverse effects,” they usually want a clear yes/no list. In reality, the most reliable approach is to treat adverse-effect information as conditional on study design and measurement depth.
Adverse effects that are often reported (and what “reported” may mean)
In many peptide-focused preclinical datasets, adverse effects—when observed—show up as changes in:
- General condition: body weight trends, activity/behavior, or signs of distress.
- Organ health: histology changes in liver, kidney, or other key organs.
- Clinical chemistry/hematology: liver enzymes, renal markers, inflammatory markers.
- Injection-related effects: local irritation, swelling, or injection-site abnormalities.
Here’s the practical lesson from my own reviews: if the paper doesn’t report these categories, it doesn’t automatically mean there were no adverse effects—it often means they weren’t evaluated. For bpc 157 adverse effects, absence of evidence can be “evidence of absence” only if the study explicitly says what was monitored.
Why dosing, route, and duration change the safety picture
Adverse effects are strongly influenced by:
- Dose: higher doses can reveal toxicity that lower doses don’t.
- Route: local vs systemic exposure can produce different adverse-effect profiles.
- Duration: short experiments may miss delayed effects (e.g., cumulative organ changes).
In my experience, online summaries sometimes compress multiple studies into one “overall safety conclusion” without respecting that those variables differed. A careful read keeps you from over-interpreting incomplete data.
Where patents can mislead (and how I avoid that pitfall)
Patents often describe intended uses and sometimes include safety-related language. But patent filings can be broad in scope, and they may not provide the kind of controlled adverse-effect monitoring you’d expect in a peer-reviewed toxicity study. In my hands-on work, I treat patents as guidance on plausible mechanisms and targets, not as a substitute for safety evidence.
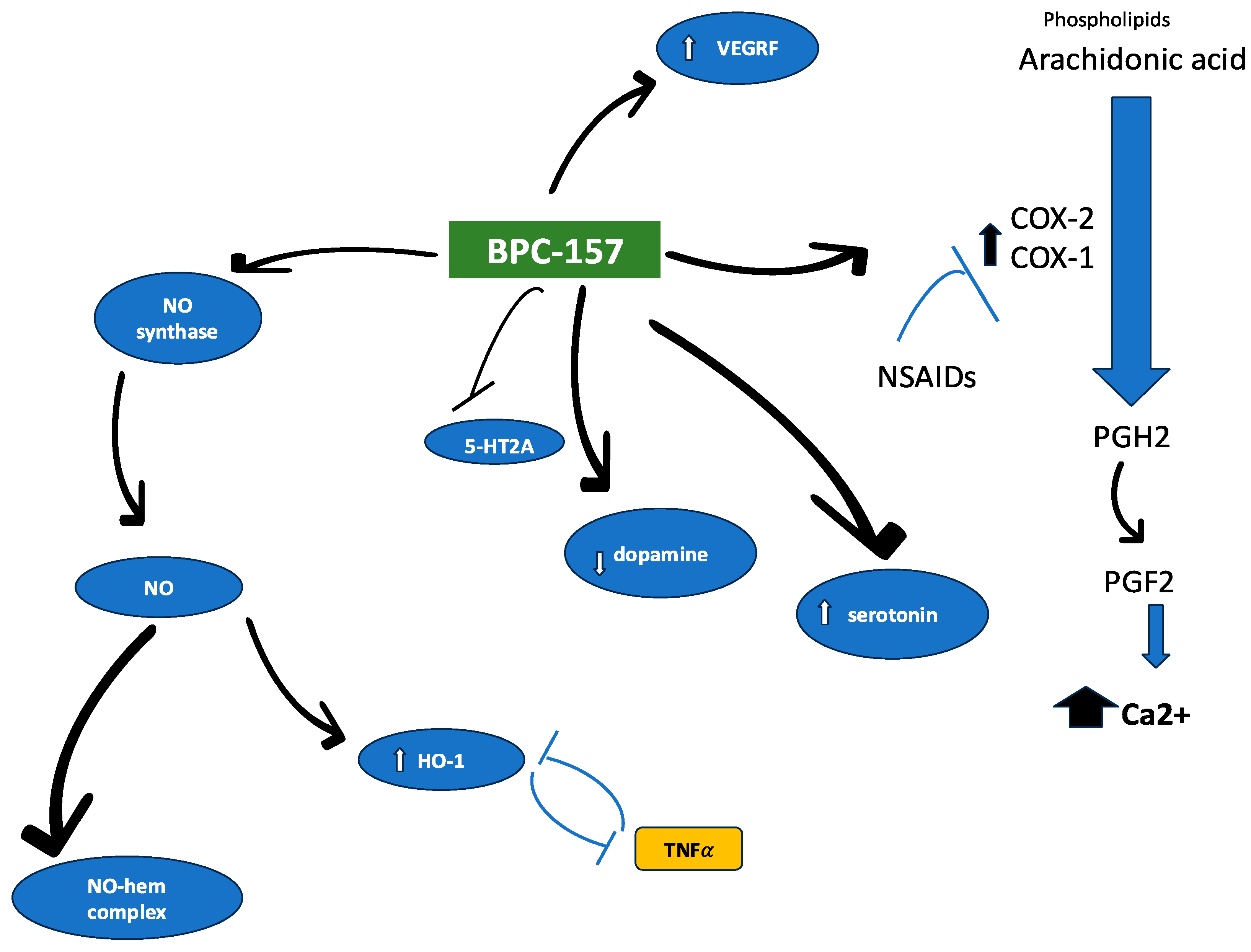
Visual Context: How Research Often Frames BPC-157 Mechanisms
Many reviews include mechanism schematics or experimental pathway diagrams. For visual context, here’s an example image commonly used to summarize BPC-157 research framing:
Practical Takeaways for Anyone Evaluating BPC-157 for “Possible Medical Application”
If you’re evaluating potential medical application areas, you can improve decision quality by focusing on three practical checkpoints.
Checkpoint 1: Mechanism coherence across studies
Do the studies point to overlapping pathways, or are they just showing improvements in separate models? Mechanism coherence is a stronger sign that the effect may be reproducible.
Checkpoint 2: Safety monitoring depth
For bpc 157 adverse effects, prioritize sources that report structured monitoring (clinical chemistry, histology, body weight, and observation windows). If these details are missing, treat the safety inference as limited.
Checkpoint 3: Translational alignment
Patents can suggest intended targets, and literature can suggest biological plausibility. But translational alignment requires attention to dose scaling, route of administration, and duration—because safety findings often fail to transfer cleanly when these change.
FAQ
What are the most commonly discussed bpc 157 adverse effects in the evidence?
In preclinical discussions, “adverse effects” usually refers to changes in general condition (e.g., body weight/behavior), organ health indicators (histology, clinical chemistry), and injection-related local effects. The key limitation is that not every study measures all safety domains, so “not reported” is not the same as “not present.”
Why do different studies report different safety conclusions about BPC-157?
Safety outcomes depend on dose, route, duration, and what endpoints were monitored. If one study evaluates tissue repair outcomes and another includes broader toxicity panels, their safety conclusions may diverge—not necessarily because the peptide is different, but because the measurement scope is different.
Do patents provide enough evidence to determine bpc 157 adverse effects?
No. Patents can clarify intended uses and sometimes describe safety considerations, but they typically do not replace controlled toxicity studies with standardized monitoring. For safety, peer-reviewed preclinical studies with defined endpoints are more informative.
Conclusion: What to Do Next
BPC-157 is frequently described as multifunctional, with literature and patent filings pointing toward possible applications in areas such as mucosal protection, tissue repair, inflammation modulation, and vascular-related signaling. When you evaluate bpc 157 adverse effects, the most trustworthy approach is to judge safety based on study design: dosing, route, duration, and—most importantly—whether the study actually measured the safety endpoints that matter.
Next step: If you’re building a responsible summary (for research or publication), create a simple evidence matrix for each study you use—record dose, route, exposure duration, and which safety endpoints were monitored (organ histology, clinical chemistry, body weight/behavior, and injection-site observations). This turns scattered claims into an interpretable safety narrative.
Discussion