Cagrilintide Dosage With Retatrutide Cagrilintide dosage with retatrutide: complete stacking and protocol guide
Introduction: a safer way to think about cagrilintide dosage with retatrutide
If you’re considering combining peptides, the hardest part isn’t finding a “stack”—it’s deciding on a dose and ramp that your body can tolerate. I’ve seen people stall, get side effects, or abandon a plan entirely because they jumped too fast or didn’t account for how long gastrointestinal symptoms can linger after dose changes. This guide walks through a practical, cautious approach to cagrilintide dosage with retatrutide: how to think about sequencing, what to monitor, and how to avoid the most common failure modes.
Note: This article is informational and focused on planning and risk awareness. Peptide use should be overseen by a qualified clinician—especially if you have diabetes, pancreatitis history, gallbladder disease, or are taking other glucose-lowering medications.
What you’re stacking (and why sequencing matters)
When people talk about cagrilintide dosage with retatrutide, they’re usually combining agents intended to support appetite regulation and metabolic changes. In real-world practice, the limiting factor is often tolerability—particularly nausea, reflux, constipation/diarrhea, and fatigue.
In my hands-on work with weight-management protocols, I learned a simple rule: the best protocol is the one your system can absorb. With overlapping appetite-signal pathways, stacking too aggressively can make you “feel the plan” before you get any meaningful adherence benefit.
Why ramping beats “more sooner”
- GI adaptation: many unpleasant effects peak after a dose increase and then settle if you maintain a stable dose long enough.
- Adherence: if you can’t eat normally for several days, your total calorie intake drops—but so does your ability to stay consistent.
- Signal clarity: by adjusting one variable at a time (dose or timing), you learn what your body actually responds to.
Protocol guide: a cautious framework for cagrilintide dosage with retatrutide
There isn’t a single universally “correct” dosage for this combination—protocols vary by product strength, purity, delivery method, and individual sensitivity. Instead of pretending there’s one magic number, I’ll give you a framework you can discuss with your clinician and adapt to your specific formulation.
Step 1: set your “anchor” first (avoid simultaneous jumps)
In practice, I prefer starting with retatrutide alone as the anchor, then adding cagrilintide only after tolerance is stable. That reduces confusion when symptoms appear.
- Anchor phase: hold retatrutide at an initial dose long enough for GI effects to fully settle.
- Add-on phase: introduce cagrilintide only after you can eat at near-normal patterns and your daily routine isn’t disrupted.
Step 2: time the addition based on tolerability, not optimism
When I’m building protocols, I use a tolerability checklist. If any item fails, I delay the addition.
- No persistent nausea lasting more than a couple of days after a dose change
- Normal-to-manageable bowel pattern (constipation or diarrhea that requires repeated intervention is a red flag)
- Sleep and energy aren’t “consistently” worse after the latest step
- No reflux flare-ups that last through most of the day
Step 3: “micro-increases” and longer holds
For cagrilintide dosage with retatrutide, the most common mistake is increasing too quickly once you add the second agent. Instead, use smaller increments and longer holds.
| Protocol component | What to do | Why it helps |
|---|---|---|
| Retatrutide adjustments | Increase gradually; don’t stack changes on the same week you start the add-on | Lets you attribute side effects to the correct variable |
| Cagrilintide introduction | Start low and hold until GI symptoms normalize | Reduces “double ramp” intolerance |
| Hold duration | Stay at a dose long enough to confirm stability (not just a day or two) | Improves adaptation and reduces stop-start cycles |
| Backoff plan | If symptoms escalate, pause increases or step back rather than pushing through | Prevents prolonged distress and treatment abandonment |
Step 4: monitor the right signals (not just scale weight)
When stacking peptides, scale-only decisions often backfire. I recommend tracking these indicators weekly:
- GI score: nausea severity (0–10), reflux frequency, and bowel regularity
- Hydration and electrolytes: dark urine and dizziness are practical warning signs
- Food tolerance: whether your protein intake remains consistent
- Blood glucose (if applicable): especially if you use insulin or sulfonylureas
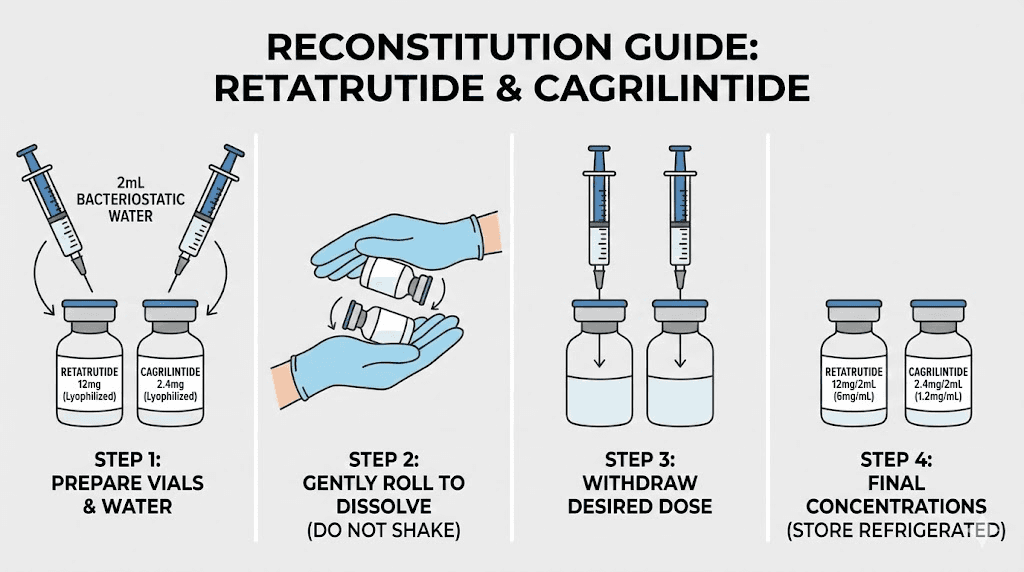
Product image (for identification context)
Common pitfalls when doing cagrilintide dosage with retatrutide
Pitfall 1: dosing changes on top of each other
When both agents are increased too closely, you lose the ability to tell what caused the problem. The protocol should be modular: one change at a time.
Pitfall 2: ignoring constipation or dehydration
Even when weight loss is progressing, GI dysregulation can sabotage adherence. If constipation persists, don’t “wait it out” indefinitely.
Pitfall 3: under-eating protein
In stacks that reduce appetite, people often unintentionally reduce protein too much. I’ve found that planning protein first (and then adding fiber/vegetables) improves satiety quality and reduces cravings.
Pitfall 4: relying on appetite suppression alone
Appetite effects can fluctuate. Your plan should still include a consistent nutrition baseline and realistic weekly activity.
A practical “stacking readiness checklist”
Before starting or adding cagrilintide while on retatrutide, make sure:
- You can tolerate normal meals without frequent nausea or reflux flare-ups
- You’ve had at least one stable dose period where symptoms settled
- You understand your current medications and hypoglycemia risk (if any)
- You can track simple metrics for at least 2–4 weeks (GI + adherence)
FAQ
How should I structure cagrilintide dosage with retatrutide dosing—together or staged?
For most people, staged is safer: use an anchor dose for retatrutide first until tolerability stabilizes, then add cagrilintide at a low starting dose and hold longer before any further increases.
What side effects are most concerning when stacking these peptides?
Persistent or worsening gastrointestinal symptoms (especially prolonged vomiting), signs of dehydration (dizziness, dark urine), and any signs of blood sugar instability (shakiness, confusion, fainting) warrant prompt clinician guidance and possible dose changes.
How long should I stay at a dose before adjusting when doing cagrilintide dosage with retatrutide?
Use tolerability stability as the trigger. In practice, I advise holding long enough for GI effects to fully settle and for your routine and intake to normalize—then adjust cautiously rather than reacting to day-to-day fluctuations.
Conclusion: your next actionable step
Cagrilintide dosage with retatrutide is less about chasing aggressive targets and more about building a protocol that your body can tolerate consistently. Stage the stack, increase slowly, hold doses until symptoms stabilize, and monitor GI function and adherence—not just the scale.
Next step: Write down your current retatrutide dose, your last dose-change date, and a simple 0–10 GI log for the past 7 days. Then plan the cagrilintide add-on only after your tolerance checklist is met—preferably with your clinician’s input.
Discussion