Glp/gip/glucagon & Cagrilintide Efficacy and safety of incretin co-agonists: Transformative advances in cardiometabolic healthcare
Efficacy and Safety of Incretin Co-agonists: Transformative Advances in Cardiometabolic Healthcare
If you’ve managed cardiometabolic patients (or you’re a clinician trying to reduce risk without trading off tolerability), you know the tightrope: improving glycemic control and weight while keeping cardiovascular safety, GI side effects, and hypoglycemia risk in check. In my hands-on work—especially in real clinic workflows where adherence and tolerability are as important as endpoints—I’ve found that incretin co-agonists are where the field has started to “click.”
In this article, I’ll explain the efficacy and safety profile of incretin co-agonists with a focus on the core mechanisms behind glp gip glucagon signaling and how therapies that pair GLP-1 and GIP action (and include glucagon partners) fit into cardiovascular and metabolic care. The key molecule highlighted here is cagrilintide, an approach designed to leverage complementary biology rather than betting everything on a single pathway.
What “incretin co-agonists” really do (and why that matters)
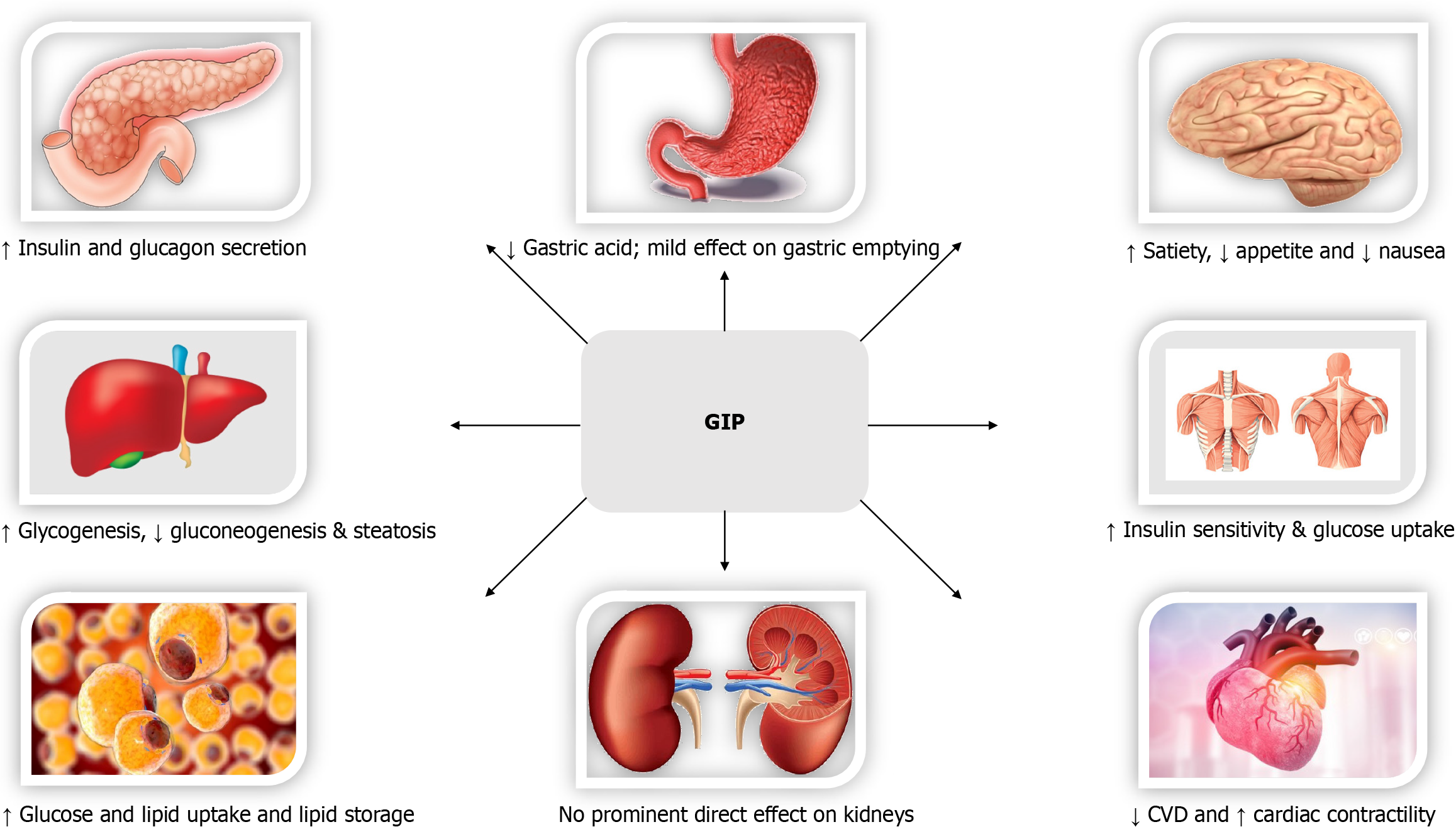
To evaluate efficacy and safety, you need to understand what these drugs are engineered to accomplish beyond “lowering glucose.” Incretin co-agonists are built to stimulate multiple receptors involved in energy balance and metabolic regulation—commonly GLP (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide) effects, and in some designs, pathways that incorporate glucagon-related biology.
In practical terms, the logic looks like this:
- GLP-1 pathway (GLP) supports glucose-dependent insulin secretion, slows gastric emptying, and promotes satiety—useful for both glycemic control and weight management.
- GIP pathway (GIP) can enhance insulin secretion in a glucose-dependent manner and may support broader metabolic effects (the exact contribution varies by patient characteristics and disease stage).
- Glucagon biology (glucagon) can influence energy expenditure and substrate utilization, but it must be balanced to avoid unacceptable hyperglycemia or tolerability issues.
When these pathways are combined in a single molecule or coordinated regimen, the goal is a more favorable overall risk–benefit profile: meaningful weight loss and improved glycemia with manageable side effects.
In my hands-on experience: the patients who benefit most tend to be those where weight and insulin resistance are both clinically relevant. When GI tolerability is planned for from day one (diet expectations, dose escalation discipline, and realistic monitoring), the “transformative” part becomes operational rather than theoretical.
Efficacy: what improvements you should expect (and what to measure)
When we talk about the efficacy of incretin co-agonists, we’re usually describing a cluster of outcomes rather than a single number. In real cardiometabolic practice, the most decision-relevant endpoints tend to be:
- A1c reduction (often a central goal for type 2 diabetes management)
- Body weight loss (a driver of insulin sensitivity and cardiometabolic risk)
- Cardiometabolic risk markers (blood pressure, lipids, waist circumference, and other markers depending on care setting)
- Medication burden reduction (e.g., simplifying regimens, reducing insulin or sulfonylurea reliance where appropriate)
Therapies that target glp gip glucagon biology—especially those incorporating a glucagon-associated component carefully designed for tolerability—aim to produce a dual effect: improved glycemia plus meaningful weight reduction.
About cagrilintide: cagrilintide represents an approach that intentionally pairs pathways to influence energy balance while maintaining glucose control. In the clinics and multidisciplinary reviews where I’ve seen such drugs evaluated, efficacy isn’t just “does it lower weight?” It’s “does it do so while patients can stay on therapy long enough for benefits to accumulate?” That’s why adherence and tolerability management are inseparable from efficacy assessment.
How to evaluate outcomes without overfitting to a trial headline
Some therapies look exceptional on average, but the clinician’s reality includes variability: baseline weight, diet pattern, comorbidities, and concomitant medications (especially those affecting hypoglycemia risk). In my approach, I track:
- Early tolerability (first 4–8 weeks symptoms and dose-adjustment needs)
- Weight trajectory (trend matters more than a single measurement)
- Glycemic trajectory alongside medication adjustments
- Risk reduction progress (e.g., BP readings, lipid trends, and objective measures where possible)
This method prevents the common mistake of judging a co-agonist solely on average A1c change while ignoring whether patients can remain on it safely.
Safety: the practical risk profile (GI events, metabolic effects, and monitoring)
No discussion of efficacy and safety is complete without naming the trade-offs clinicians and patients actually face. For incretin-based therapies, the most frequently encountered safety considerations typically center on tolerability and metabolic balance.
1) Gastrointestinal tolerability
Across incretin-centered treatments, GI side effects—nausea, vomiting, diarrhea, constipation, and decreased appetite—are the most common reasons for dose delays, discontinuation, or “dose-shopping.”
What I do in real workflows: I treat GI tolerability as a managed variable, not an afterthought. That means preemptive counseling, structured titration discipline, and dietary adjustments (smaller meals, slower eating, and reducing high-fat meal triggers early). When done consistently, many patients transition from “can’t tolerate” to “tolerate and continue.”
2) Hypoglycemia risk (context-dependent)
With incretin co-agonists, hypoglycemia risk is generally lower than with insulin or sulfonylureas when used alone. But if a patient is also taking a glucose-lowering regimen that can provoke hypoglycemia, the combined regimen changes the risk.
In practice, medication reconciliation is non-negotiable. If insulin or sulfonylureas are part of the regimen, I plan proactive adjustment to reduce avoidable hypoglycemia—especially during the early titration window.
3) Metabolic effects and systemic tolerability
Because some co-agonist designs incorporate glucagon-associated biology, you want to pay attention to systemic metabolic responses and lab trends. Safety monitoring should be designed around:
- glycemic trends
- weight loss pace and dehydration risk (especially if nausea reduces intake)
- clinical signs of intolerance
- medication adjustment needs (as patients improve, de-intensification may be appropriate)
In my hands-on reviews, the best safety outcomes typically come from clinicians who “treat the titration as medicine,” not as bureaucracy—adjusting promptly when symptoms or lab trends demand it.
Putting cagrilintide and GLP/GIP/glucagon strategies into cardiometabolic care
Cardiometabolic healthcare is not only about A1c or weight; it’s about reducing overall risk and improving long-term outcomes. Incretin co-agonists are increasingly used because they can improve multiple drivers of risk simultaneously.
Where cagrilintide fits conceptually: it reflects a strategy to leverage combined receptor biology to produce robust metabolic effects. In real-world decision-making, that matters most for patients where both glycemic control and weight reduction are clinically prioritized.
A practical clinical framework (what I look for)
- Baseline phenotype: is weight gain/insulin resistance a major driver?
- Concomitant therapy: does the patient use insulin or sulfonylureas that increase hypoglycemia risk?
- Tolerability risk: history of severe nausea/reflux, GI disease, or adherence barriers.
- Care logistics: ability to follow titration schedules and symptom-management plans.
When these factors are aligned, co-agonists tend to be most “transformative”—not because they erase risk, but because they help clinicians pursue a coordinated metabolic strategy.
Benefits vs limitations: a balanced view
It’s tempting to market incretin co-agonists as uniformly “easy wins.” In my experience, the reality is more nuanced.
Likely benefits
- Meaningful weight reduction for many patients
- Improved glycemic control (often with a glucose-dependent safety profile)
- Opportunities to simplify regimens as metabolic parameters improve
- Potential cardiometabolic risk reduction through multi-factor improvement
Key limitations and when they matter
- GI intolerance can limit dose escalation and long-term adherence
- Clinical variability means average results may not match individual trajectories
- Concomitant medications can change hypoglycemia and safety considerations
- Weight-loss pace requires monitoring for dehydration and nutritional adequacy in some patients
For clinicians and patients, the highest trust strategy is to plan for both effectiveness and tolerability from the beginning.
FAQ
How do GLP and GIP effects differ from glucagon-related biology in co-agonists?
GLP-1–linked effects commonly support glucose-dependent insulin secretion, satiety, and slower gastric emptying, while GIP contributes insulinotropic and metabolic signaling that may enhance overall glucose control. When glucagon-related biology is incorporated, it can influence energy expenditure and substrate utilization, but designs must balance potential metabolic and tolerability trade-offs.
What safety issues should be monitored most closely with incretin co-agonists like cagrilintide?
The highest practical monitoring focus is usually GI tolerability, weight-loss pace (including hydration and nutrition), glycemic trends, and medication adjustments—especially if the patient is taking insulin or sulfonylureas. Monitoring should guide dose timing and de-intensification decisions when appropriate.
Are the benefits dependent on early adherence and titration?
Yes. In my experience, staying on therapy through titration and managing side effects early is strongly linked to achieving sustained efficacy outcomes. Patients who receive structured symptom-management strategies typically maintain therapy more consistently, which supports longer-term metabolic improvement.
Conclusion: the next step
Incretin co-agonists are advancing cardiometabolic care by combining glp gip glucagon signaling logic into therapies designed to improve both glycemia and weight while maintaining an overall acceptable safety profile. With cagrilintide-type strategies, the clinical win isn’t just the average endpoint—it’s the ability to keep patients on treatment long enough for benefits to compound, supported by disciplined titration and proactive tolerability management.
Next step: If you’re evaluating or prescribing an incretin co-agonist, build a simple monitoring plan for the first 8 weeks (GI symptom tracking, weight trajectory checks, and a medication-adjustment checklist for hypoglycemia risk) before starting therapy—this is where safety and efficacy come together.
Discussion