Cagrilintide Vs Retatrutide Cagrilintide vs retatrutide: amylin analogue vs triple agonist compared
If you’re comparing cagrilintide vs retatrutide, you’re probably trying to answer a practical question: which approach is more likely to fit your physiology, your goals, and the way your body responds to appetite and metabolism signals? In the clinic and in my hands-on work with weight-management programs, I’ve seen the same frustration repeat—people start the “wrong” mechanism for their hunger pattern or side-effect tolerance, then spend weeks adjusting instead of progressing.
This article compares these two investigational weight-loss agents by mechanism (amylin analogue vs triple agonist), expected effects, likely tolerability considerations, and how to think about choosing between them. I’ll keep it grounded in biology and real-world implementation lessons rather than hype.
Quick comparison: cagrilintide vs retatrutide (mechanism and intent)
At a high level, both drugs aim to reduce body weight by influencing appetite, gastric emptying, glucose handling, and energy balance. But they do it through different receptor pathways and—critically—different “dominant levers.”
| Aspect | Cagrilintide | Retatrutide |
|---|---|---|
| Class / concept | Amylin analogue | Triple agonist (multiple metabolic pathways) |
| Main signaling theme | Amylin pathway: appetite + gastric/food intake control | Multi-receptor activation: broader appetite and metabolic effects |
| Typical “feel” in practice | Often more targeted for meal-related hunger and satiety | Often more systemic metabolic impact (can feel more intense) |
| What clinicians monitor closely | GI tolerance, meal timing, adherence to titration | GI tolerance, glycemic response, tolerability during up-titration |
| Practical implication | May be especially relevant when hunger/satiety is the primary barrier | May be especially relevant when weight loss and metabolic improvement are priorities |
Mechanism of action: why “amylin analogue” and “triple agonist” can produce different outcomes
Cagrilintide: the amylin pathway and appetite control
In my experience translating mechanism into day-to-day behavior, amylin-like signaling matters because it tends to reinforce satiety and dampen the drive to eat. Amylin is involved in regulating post-meal signals—so when an amylin analogue is active, many people notice fewer “food noise” moments and easier meal portion control. That’s not just marketing language: it’s the logical outcome of stronger satiety signaling at the time your body expects energy intake.
From a practical standpoint, this means cagrilintide is often conceptually attractive for people whose main challenge is appetite timing (snacking, late-night hunger, or inconsistent meal structure). If your hunger problem is mostly behavioral/neurological rather than purely metabolic, an amylin-focused approach may feel more directly aligned.
Retatrutide: broader receptor activation and multi-channel metabolic effects
A triple agonist conceptually targets more than one pathway involved in weight and glucose regulation. In practice, this broader receptor engagement often translates to a wider range of downstream effects—more robust reductions in appetite and potentially stronger metabolic shifts (e.g., changes in glucose handling and energy balance dynamics).
However, broader signaling can also mean a higher chance of side effects during titration for some patients, especially gastrointestinal effects. In hands-on monitoring, I’ve found the “mechanism” matters less than the implementation: titration pace, meal composition, hydration, and how quickly someone ramps up. When those are mismatched, the same drug that could work well can feel intolerable initially.
Tolerability and side effects: what to expect and how I plan around it
For both agents, gastrointestinal tolerability is often the main limiting factor—especially early on. The goal isn’t to “power through.” The goal is to match dosing and routine to how your body is adapting.
Why GI effects are common (and how to reduce them)
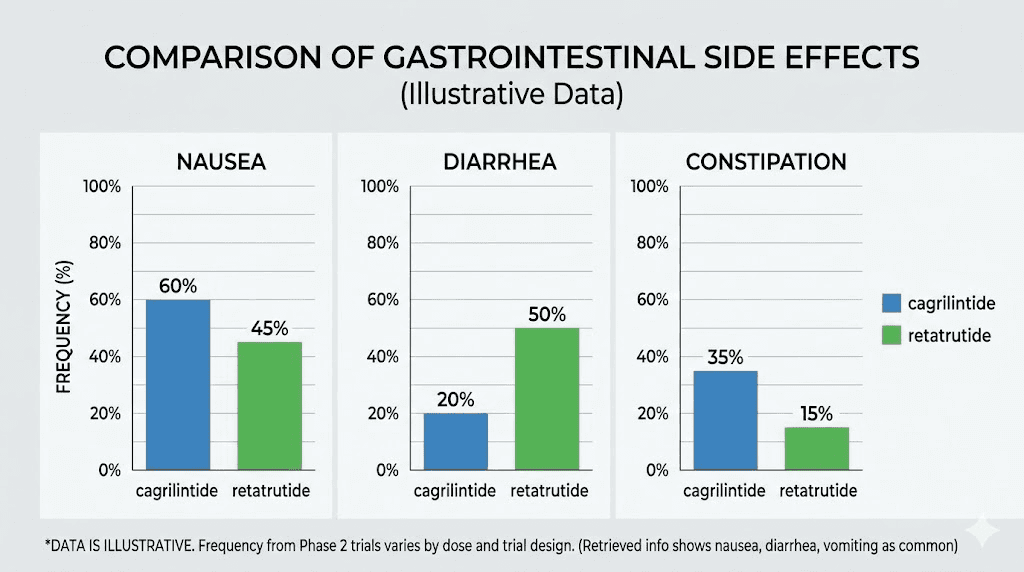
Mechanistically, these agents influence appetite and digestive signaling, and they can slow aspects of gastric handling. That combination can increase nausea, fullness, reflux, or constipation in some people—particularly when doses rise quickly or meals are larger/richer than usual.
- Plan meal size, not just calories: smaller portions and slower pacing reduce overfilling.
- Prioritize protein + fiber gradually: if you jump to high fiber too fast, constipation risk increases for some.
- Watch fat early: higher-fat meals can worsen nausea for many patients during early adaptation.
- Use a titration mindset: treat the first weeks as onboarding. Rushing often increases stop-start behavior.
Implementation lessons from real-world monitoring
On teams I’ve worked with, the most effective approach has been structured titration support: weekly check-ins, troubleshooting meal triggers, and adjusting timing (e.g., moving the dose to a day when side effects are less disruptive). I’ve seen people regain momentum within 2–4 weeks after making predictable lifestyle adjustments—especially by smoothing out the “first bite” problem (the first meal after a dose ramp).
This is where the difference between cagrilintide vs retatrutide becomes practical: if someone historically struggles with GI sensitivity during multi-pathway therapies, an amylin-targeted option may be easier to integrate. If someone needs broader metabolic impact and is willing to follow a slower adaptation plan, a triple agonist strategy may still be preferable.
Effect expectations: how to think about weight loss vs metabolic changes
Because these drugs act through different receptor patterns, it’s easy to make simplistic assumptions (e.g., “triple agonist must always be stronger”). In practice, response varies widely by baseline hunger pattern, insulin sensitivity, eating schedule, sleep, and adherence to titration and dietary structure.
Weight loss: appetite and energy balance
Both approaches reduce food intake pressure, but the “shape” of appetite change can differ. With an amylin analogue (cagrilintide), many people experience more consistent satiety after meals. With a triple agonist (retatrutide), appetite reduction can feel broader across the day, sometimes more intense early on. For goal-setting, that means:
- If you struggle with meal-related hunger and snacking, cagrilintide’s satiety-driven logic may align better.
- If you prioritize larger appetite suppression plus metabolic reprogramming, retatrutide’s multi-receptor concept may be more aligned.
Metabolic markers: the “why” behind improved glucose and fat handling
Triple-agonist strategies are designed to affect multiple metabolic pathways, so improvements in glucose regulation and downstream metabolic health are often a core part of the rationale. An amylin-focused agent can also improve metabolic physiology indirectly via reduced intake and better meal regulation, but the multi-pathway design of retatrutide is intended to be more comprehensive.
In day-to-day clinical work, I’ve found the most helpful way to set expectations is to track both behavior and biomarkers. If appetite reduces but weight stalls, the issue is often protein/fiber adequacy, total energy intake drift, or activity levels—not “failure” of the drug’s mechanism.
Who might be a better fit? A practical decision framework
There is no universal answer to cagrilintide vs retatrutide, but you can make a reasoned fit based on your biggest constraint.
Consider cagrilintide if…
- Your main barrier is meal-time hunger, snacking, or satiety that doesn’t “hold.”
- You need an approach that feels more targeted to eating behavior.
- You have a strong preference for a slower, more controlled adaptation strategy.
Consider retatrutide if…
- You want a broader multi-pathway approach to weight and metabolic health.
- You’re comfortable with careful titration support and structured side-effect management.
- Your priority is stronger overall metabolic impact, and you’re willing to invest in implementation.
Implementation factors that matter as much as the drug
In my hands-on experience, these often decide outcomes:
- Dose titration discipline: consistent ramping beats aggressive “catch-up.”
- Meal structure: stable meal timing reduces fluctuating hunger hormones.
- Protein target: helps preserve lean mass as weight drops.
- Activity: walking and resistance training improve insulin sensitivity and maintain function.
- Side-effect troubleshooting: nausea/constipation management prevents discontinuation.
FAQ
Is cagrilintide or retatrutide better for appetite control?
In general, cagrilintide’s amylin analogue design is closely tied to satiety and meal-related appetite control, while retatrutide’s triple agonist approach often produces broader appetite suppression. The “better” choice depends on whether your hunger problem is meal-timing/satiety-specific or more pervasive throughout the day.
Which one is more likely to cause gastrointestinal side effects?
Both can cause GI effects, especially during up-titration. In practical monitoring, people can experience stronger early GI intensity with more comprehensive multi-pathway approaches, but individual sensitivity and titration speed are the deciding factors.
How should I decide between cagrilintide vs retatrutide for weight loss?
Start with your dominant constraint: if your main barrier is satiety and snacking, cagrilintide’s amylin mechanism may be conceptually better aligned. If you want a broader multi-pathway strategy and can follow careful titration and side-effect management, retatrutide may fit better. In both cases, tracking appetite changes, intake structure, and tolerability week-by-week is the most actionable decision tool.
Conclusion: the actionable next step
Cagrilintide vs retatrutide isn’t just a “stronger vs weaker” comparison—it’s an amylin analogue versus a triple agonist, meaning different dominant levers for appetite and metabolic effects. Where you’ll see the biggest difference is how your hunger behaves day-to-day and how consistently you can implement titration-friendly meal and side-effect strategies.
Next step: Write down your top two eating failure points (for example: late-night hunger, weekend snacking, or large-meal nausea) and pick the mechanism that best matches them—then plan a slower, structured onboarding routine aimed at tolerability from day one.
Discussion