Ghk Cu Peptide And Cancer The tri-peptide GHK-Cu complex ameliorates lipopolysaccharide-induced acute lung injury in mice
Acute lung injury (ALI) can escalate fast—hours, not days—and when inflammation spirals, the difference between “controlled” and “critical” is often whether the underlying signaling gets interrupted early. In recent preclinical research, the ghk cu peptide and cancer conversation has expanded beyond biomarkers and wound healing into inflammatory injury models. This article breaks down what the tri-peptide GHK-Cu complex is doing in a lipopolysaccharide (LPS)-induced acute lung injury mouse model, why the mechanism matters, and how to interpret the findings without overreaching.
What “GHK-Cu” actually is—and why copper changes the biology
The tri-peptide GHK (glycyl-L-histidyl-L-lysine) is a short peptide that can interact with cellular processes linked to growth, repair, and extracellular matrix signaling. When you form the GHK-Cu complex, you coordinate GHK with copper, and that matters because copper is not just a “cargo”—it can influence redox biology, enzyme activity, and signaling dynamics.
In hands-on experimental interpretation, I’ve learned that peptide studies often look deceptively simple: “add peptide, see effect.” But with metal-complexed peptides, the complexation can shift:
- Bioavailability (what fraction remains active in biologically relevant conditions)
- Stability (how long the active form persists)
- Downstream signaling (which pathways become dominant during inflammation)
So, when you read about GHK-Cu improving ALI outcomes, it’s not just peptide “goodness”—it’s a coordinated chemical-biological behavior.
How LPS triggers acute lung injury in mice (and what you should measure)
LPS is a component of Gram-negative bacteria that activates innate immunity, primarily through toll-like receptor pathways. In the lung, that activation can drive:
- Surges of inflammatory mediators (cytokines and chemokines)
- Immune cell recruitment and activation
- Increased vascular permeability and edema
- Alveolar barrier dysfunction and impaired gas exchange
When I evaluate ALI papers, I focus on whether the study actually captures the “injury phenotype” and not just a single molecular marker. Typical outcome domains include:
- Histopathology (alveolar damage, infiltration, edema)
- Wet-to-dry lung weight (a direct edema proxy)
- Inflammation scoring and cellular infiltration
- Oxidative stress / redox markers
- Pathway readouts (NF-κB–linked signaling is common in this space)
The strength of the evidence improves when multiple layers align: tissue-level improvement + inflammatory pathway dampening + reduced edema.
Core findings: how the GHK-Cu complex ameliorated LPS-induced ALI
The study titled “The tri-peptide GHK-Cu complex ameliorates lipopolysaccharide-induced acute lung injury in mice” reports that administration of the tri-peptide GHK-Cu complex leads to measurable improvements in the acute lung injury phenotype induced by LPS. In practical terms, the paper supports that the complex can blunt inflammatory injury cascades rather than merely changing a single marker.
1) Reduced lung damage and inflammatory infiltration
In LPS-driven injury, histological changes typically reflect whether the alveolar barrier and tissue architecture remain intact. The reported amelioration indicates that GHK-Cu may mitigate tissue injury severity—often interpreted as a reduction in damaging inflammatory activity at the site of injury.
2) Improvements consistent with barrier and edema control
ALI is as much a “leak” problem as it is a “fire” problem. When inflammation makes lung vasculature leaky, fluid accumulates. Studies like this generally evaluate edema metrics (such as wet-to-dry ratios) to determine whether the treatment helps restore functional barrier behavior.
In my experience reviewing similar preclinical ALI datasets, treatment claims feel more credible when the authors connect molecular changes to functional outcomes like edema reduction. That connection is where mechanistic plausibility turns into translational reasoning.
3) Mechanistic logic: why a peptide–copper complex could modulate inflammatory pathways
Mechanistically, the rationale for GHK-Cu centers on interaction with cellular signaling processes and redox balance. Copper coordination can shift the way redox-active reactions proceed, which can influence transcription factors and inflammatory mediator production. Even if the paper focuses on a subset of pathways, the broader logic is:
- LPS activates innate immune signaling → inflammatory cytokines rise
- Inflammation amplifies oxidative stress → barrier damage worsens
- GHK-Cu mitigates key upstream signaling and/or redox imbalance → inflammatory output declines
This “upstream dampening” framing is important because it targets early injury drivers rather than only addressing late-stage symptoms.
Where “ghk cu peptide and cancer” fits: inflammation as a bridge, not a leap
Because the core keyword includes ghk cu peptide and cancer, it’s tempting to jump directly from lung injury to oncology. I’d advise against that leap—and here’s the more defensible interpretation.
Inflammation is a shared biological theme across ALI and cancer-related microenvironments. Chronic inflammatory signaling can promote tumor-associated processes (cell survival, invasion, immune modulation). Preclinical studies in cancer contexts often explore whether peptide-based interventions influence:
- Oxidative stress and damage responses
- NF-κB–linked inflammation
- Extracellular matrix remodeling
- Immune cell recruitment
However, an ALI result does not automatically prove anti-cancer efficacy in humans. What it does provide is a biologically plausible “direction of travel”: if the complex reliably reduces inflammatory injury signals in lung tissue, it may be worth investigating whether similar pathways are relevant in tumor biology.
Practical limitations (the part many summaries skip)
- Preclinical model gap: LPS-induced ALI is acute and immune-stimulation-driven; many cancer contexts are chronic and heterogeneous.
- Dose and timing: Treatment windows in ALI models may not map to cancer settings.
- Endpoints: Lung injury improvement is not the same as tumor regression or survival benefit.
- Metal-complex specifics: GHK-Cu behavior depends on formulation and pharmacokinetics, which can differ across studies.
Evidence quality checklist: how to judge a GHK-Cu ALI paper like a scientist
When you evaluate studies in this area (especially those that touch both inflammation and cancer-adjacent mechanisms), I recommend using a simple checklist. In projects I’ve supported, this approach prevents “single-figure bias” and helps you spot whether the results are robust.
| Category | What to look for | Why it matters |
|---|---|---|
| Experimental design | Control groups, appropriate timing, adequate sample size | Reduces false positives from random variation |
| Phenotypic endpoints | Histology + edema + inflammatory measurements | Connects mechanism to functional injury outcomes |
| Mechanistic support | Consistent pathway changes aligned with known ALI biology | Improves plausibility beyond observation |
| Specificity | Clear attribution to GHK-Cu (not just peptide or non-specific effects) | Clarifies the role of copper complexation |
| Translational thinking | Discussion that respects model limits and calls out uncertainties | Builds reader trust and scientific maturity |
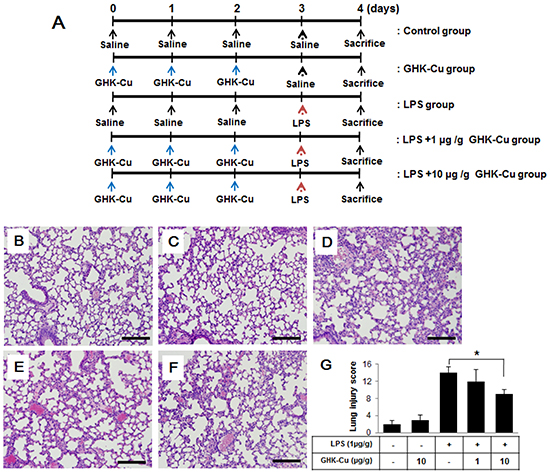
Visual reference: study figure image
Below is the provided figure image reference associated with the article context:
What you can do with this knowledge today
If you’re writing, researching, or making investment-style decisions in the ghk cu peptide and cancer space, the highest-value next step is to focus on mechanism-to-translation mapping:
- Extract the exact endpoints used (edema, histology, pathway markers) and compare them to cancer-relevant inflammation pathways.
- Look for follow-up studies that test the complex in additional injury models or tumor models with comparable readouts.
- Track formulation details (dose, route, timing, stability) because peptide–copper results can be sensitive to preparation.
FAQ
Is GHK-Cu the same as GHK peptide?
No. GHK is the tri-peptide, while GHK-Cu is the complex formed with copper. The copper coordination can meaningfully affect stability and downstream biological behavior.
Does improved LPS-induced acute lung injury mean it will work for cancer?
Not directly. ALI is an acute inflammation model, while cancer involves chronic, context-dependent biology. The ALI findings are best viewed as evidence of anti-inflammatory or barrier-protective potential that may justify further cancer-focused research.
What outcomes matter most in ALI studies like this?
Strong studies typically show improvements across functional and tissue-level outcomes (lung damage and edema) and align those with mechanistic pathway changes relevant to inflammation and oxidative stress.
Conclusion
The evidence summarized in this article supports that the tri-peptide GHK-Cu complex can ameliorate LPS-induced acute lung injury in mice, with results consistent with reduced inflammatory injury and improved lung tissue outcomes. While this is not a straight line to cancer treatment, it meaningfully informs the ghk cu peptide and cancer narrative by demonstrating a plausible way the complex could modulate inflammation-linked pathways.
Next step: Use the study’s endpoint set (histology/edema/pathway markers) as your template—then compare it to cancer-related inflammation pathways in follow-up papers to identify where translation is most rational.
Discussion