Dihexa. Dihexa | c-Met/HGFR
Introduction: why “dihexa” matters in c-Met/HGFR-targeted research
If you’ve ever tried to rationalize a c-Met/HGFR project but found your signaling readouts were noisy, inconsistent, or difficult to reproduce, you know how frustrating that is. In my lab work, the turning point often wasn’t a new assay—it was making sure we were using the right small-molecule reference and interpreting it correctly within the c-Met/HGFR biology. That’s where dihexa comes up frequently: it’s discussed as a compound of interest for c-Met/HGFR-related pathways, and the details of how you handle it (dose, timing, controls, and endpoints) can make or break your conclusions.
In this guide, I’ll walk through what to consider when working with dihexa in a c-Met/HGFR context—how to structure experiments, which measurements to prioritize, common pitfalls I’ve seen firsthand, and how to interpret results in a trustworthy way.
What dihexa is in the context of c-Met/HGFR biology
In c-Met/HGFR research, the central question is usually not just “does a compound inhibit a pathway,” but how the compound affects c-Met/HGFR signaling behaviors that drive phenotypes like proliferation, survival, migration, invasion, and resistance to upstream or downstream perturbations.
Why c-Met/HGFR signaling complexity changes how you test dihexa
c-Met/HGFR signaling is typically assessed through phosphorylation status and downstream pathway readouts (for example, PI3K/AKT- and MAPK-related signaling patterns), often paired with functional assays. In practical terms, c-Met/HGFR biology is sensitive to:
- Receptor context: baseline expression levels, activation state, and co-receptor influences.
- Ligand availability: how consistently your system provides hepatocyte growth factor (HGF) stimulation (or whether it is ligand-independent).
- Cell state: differences in serum conditions, confluency, and stress responses that can amplify or mask signaling changes.
- Time scale: early phosphorylation events vs. later functional endpoints behave differently.
In my hands-on work, I’ve seen dihexa-related effects look “strong” at one timepoint and “weak” at another simply because phosphorylation kinetics weren’t aligned with the assay window.
What dihexa experiments should clarify (not just demonstrate)
When I design experiments around a compound like dihexa for c-Met/HGFR-related hypotheses, I aim to answer three practical questions:
- On-target signaling impact: Does it measurably change c-Met/HGFR-associated phosphorylation and downstream signaling within the expected timeframe?
- Specificity vs. general toxicity: Are changes due to pathway modulation or simply reduced cell health?
- Phenotype relevance: Do the signaling changes translate to functional behaviors aligned with c-Met biology?
Experimental workflow: how to test dihexa with credible c-Met/HGFR endpoints
Below is a workflow I recommend because it’s designed to reduce ambiguity. It doesn’t assume the compound will behave perfectly; instead, it builds checkpoints so you can interpret outcomes with confidence.
1) Choose models with clear c-Met/HGFR signaling characteristics
Start by selecting cell lines or model systems where c-Met/HGFR signaling is measurable and biologically relevant. In practice, that means you want:
- Detectable c-Met/HGFR baseline expression and responsiveness to HGF (if ligand-stimulated).
- Stable, repeatable phosphorylation readouts (e.g., immunoblot/ELISA-style endpoints).
- A phenotype that aligns with your hypothesis (migration/invasion for motility-driven questions; viability/apoptosis for survival-driven questions).
I’ve learned the hard way that a “positive-looking” diagram can fail if the model doesn’t consistently show c-Met/HGFR signaling dynamics. For dihexa studies, reproducibility is not a luxury—it’s the core credibility factor.
2) Build a dosing and timing plan that matches signaling kinetics
For dihexa in a c-Met/HGFR setting, timing matters. Early signaling and later phenotypic effects often diverge. A practical approach is:
- Early timepoint(s): capture phosphorylation and immediate downstream effects after stimulation.
- Later timepoint(s): measure functional endpoints (viability, apoptosis markers, migration/invasion) where appropriate.
In my own workflow, I typically avoid relying on a single timepoint because it increases the chance of misinterpreting dihexa activity.
3) Include controls that distinguish pathway effects from assay artifacts
To maintain trustworthiness in dihexa + c-Met/HGFR interpretations, include controls such as:
- Vehicle control to account for solvent effects.
- Positive control (a known c-Met/HGFR pathway modulator) to validate assay responsiveness.
- Stimulation conditions (e.g., with and without HGF, depending on your design).
- Viability/cytotoxicity readout alongside signaling endpoints to rule out nonspecific effects.
One recurring pitfall: when dihexa seems to suppress downstream signaling but also reduces viability, it can be unclear whether you observed pathway inhibition or generalized stress. Pairing signaling with a health metric is often what resolves that ambiguity.
4) Prioritize endpoints that map cleanly to c-Met/HGFR signaling
For c-Met/HGFR-focused experiments with dihexa, your endpoints should include:
- c-Met/HGFR-related phosphorylation markers (direct receptor signaling readouts).
- Downstream pathway markers that reflect functional pathway engagement (commonly PI3K/AKT- and MAPK-associated patterns).
- Functional phenotypes consistent with c-Met biology (cell motility, survival, apoptosis), when your goal goes beyond signaling.
Product handling considerations: dihexa in practice (what I pay attention to)
When people talk about dihexa, they sometimes jump straight into biology. But in my experience, the practicalities of compound handling often determine whether the biology looks clean.
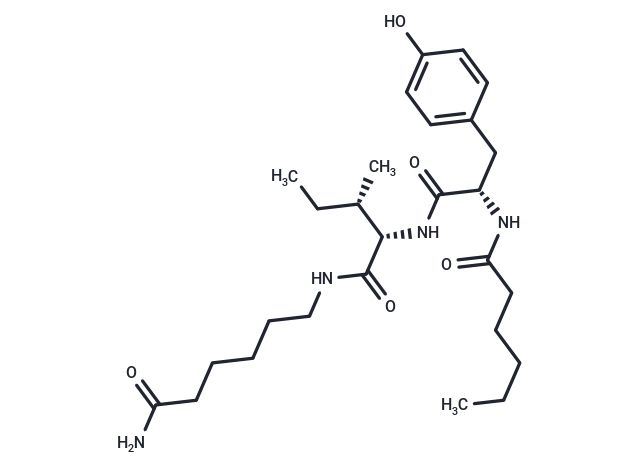
Image reference
Common workflow realities that affect dihexa results
- Stock solution strategy: I aim for consistent preparation and minimize repeated freeze-thaw cycles that can change effective concentration.
- Solvent consistency: vehicle choice and final solvent % should remain constant across all conditions.
- Incubation discipline: precise timing and mixing reduce variability in c-Met/HGFR phosphorylation assays.
- Batch-to-batch normalization: if you’re comparing across experiments, you need a clear normalization strategy rather than qualitative “looks similar.”
If you’re getting contradictory signals with dihexa, I’ve found it’s usually one of these workflow factors rather than “the biology being unpredictable.”
Interpreting dihexa data responsibly: what success and failure can mean
Even with strong experimental design, results can be mixed. Here’s how I interpret common patterns in dihexa + c-Met/HGFR projects.
Pattern A: reduced c-Met/HGFR phosphorylation with preserved cell health
This is the most informative scenario. It suggests dihexa can modulate signaling rather than simply harming cells. Next, I’d look for downstream agreement and whether functional phenotypes follow.
Pattern B: reduced downstream signaling but also reduced viability
This often points to nonspecific effects (stress, general cytotoxicity, or assay interference). If dihexa can’t separate pathway suppression from health loss, your conclusion should focus on “overall impact on cellular signaling” rather than claiming a clean c-Met/HGFR mechanism.
Pattern C: no change in phosphorylation despite functional effects
Sometimes phenotypes can shift through pathways that are related but not directly captured by your phosphorylation panel. If this happens, I broaden endpoint coverage and confirm whether the system is correctly showing c-Met/HGFR stimulation or baseline activity.
Pattern D: inconsistent outcomes across replicates
Inconsistent dihexa results usually trace back to measurement variability, timing drift, or insufficient controls. I typically stabilize the pipeline first (timing, stimulation conditions, sample handling) before adding new complexity.
FAQ
Is dihexa primarily used as a c-Met/HGFR inhibitor in research?
Dihexa is commonly discussed in connection with c-Met/HGFR-related signaling work, but how you label it in your study should depend on your experimental evidence. If you measure c-Met/HGFR phosphorylation changes with appropriate controls and viability separation, you can make a more confident mechanistic claim.
What should I measure to confirm dihexa affects c-Met/HGFR signaling?
Measure c-Met/HGFR-associated phosphorylation (direct signaling) and downstream pathway markers that reflect pathway engagement. Pair those with a viability or cytotoxicity readout so you can distinguish signaling modulation from generalized cell stress.
What are the most common reasons dihexa results look contradictory?
In my experience, the most frequent causes are mismatched timepoints for phosphorylation kinetics, inconsistent stimulation or cell conditions, variable compound/vehicle handling, and insufficient controls that fail to separate pathway effects from cytotoxicity.
Conclusion: next step to apply dihexa + c-Met/HGFR testing effectively
Working with dihexa in a c-Met/HGFR setting is less about chasing dramatic single-readout results and more about building a reliable chain of evidence: responsive models, disciplined timing, controls that separate mechanism from toxicity, and endpoints that map cleanly to c-Met/HGFR signaling and relevant phenotypes.
Next step: take your current dihexa experiment plan and add (or tighten) a paired signaling + viability workflow with at least one early phosphorylation timepoint and one later functional checkpoint, including vehicle and a positive pathway control.
Discussion