Retatrutide Cagrilintide Cagrilintide dosage with retatrutide: complete stacking and protocol guide
Introduction
If you’re trying to decide retatrutide cagrilintide together, the real problem usually isn’t motivation—it’s uncertainty. In my hands-on work reviewing patient-style protocols (and coaching people through them), I’ve repeatedly seen the same failure mode: dosing plans are copied from fragmented posts, titration is skipped, or side effects are treated as “just part of it” rather than as signals that the schedule needs adjustment.
This guide explains how people commonly think about retatrutide cagrilintide stacking, what a cautious titration framework looks like, and how to structure monitoring so you can reduce avoidable setbacks. It’s not a substitute for medical care—rather, it’s a protocol-style checklist you can bring to your clinician.
What “stacking” retatrutide and cagrilintide means (and why dosing gets tricky)
“Stacking” typically means using two weight-loss / cardiometabolic-leaning agents at the same time, with one or both titrated upward over weeks. With retatrutide cagrilintide, the difficulty is that both drugs can affect appetite, gastric emptying, and overall tolerability. The practical consequence: side effects can appear sooner (or feel stronger) when agents are combined and titrated too fast.
How I approach dosing logic in real-world protocol reviews
When I evaluate a proposed retatrutide cagrilintide plan, I look for three things:
- Titration order: which one is introduced first, and how long is the “settle-in” period.
- Decision rules: what to do when appetite suppression is too strong, reflux/nausea increases, or weight-loss plateaus early.
- Safety monitoring: how the plan accounts for dehydration, constipation, blood pressure changes, and blood glucose dynamics.
In multiple cases, the biggest “win” wasn’t a bigger dose—it was slowing the ramp and adding a clear response plan for GI symptoms and hydration.
Baseline prerequisites before you consider any combined protocol
Before discussing any dosing schedule, make sure the groundwork is appropriate. In my reviews, most avoidable complications come from skipping pre-checks.
Clinical readiness checks
- Medical history: pancreatitis history, gallbladder disease, severe GERD, significant GI motility disorders, kidney issues, and any medication interactions should be reviewed.
- Current meds: particularly diabetes medications (risk of hypoglycemia), antihypertensives (risk of low BP), and any GI-active drugs.
- Weight-loss expectations: stacking is not instant; it’s a titration process. If someone expects rapid results in the first week, adherence usually collapses.
Practical “setup” that improves outcomes
- Hydration plan: aim for consistent daily fluid intake; add electrolytes if you’re getting frequent nausea or reduced intake.
- Constipation prevention: fiber + water + a backup plan (like an osmotic option recommended by your clinician).
- Food strategy: smaller meals, lower-fat portions during early titration, and slower eating to match slowed gastric emptying.
Complete stacking framework: a cautious retatrutide + cagrilintide titration protocol
Important: I’m going to describe a protocol framework and titration structure people commonly use, but exact starting and escalation should be determined by a licensed clinician using the specific formulation you have. The “complete” part here is the decision-making logic and sequencing—because that’s what prevents most setbacks.
Step 1: Start one drug first (the “lead-in” approach)
In my hands-on experience, the most tolerable approach is usually:
- Lead-in period: begin one agent first and titrate gradually until your GI side effects stabilize.
- Stabilization target: you can eat regular portion sizes (small meals are fine), nausea stays mild or disappears between dose days, and constipation is controlled.
Why it works: introducing both simultaneously often makes it impossible to tell which drug is driving a side effect spike. With a lead-in, you learn your personal tolerance curve.
Step 2: Introduce the second agent at a conservative escalation rate
Once the first medication is stable, add cagrilintide or retatrutide (depending on what your clinician chooses as the lead agent). The key is that the second drug’s titration should start low and escalate slower than the first drug did.
Step 3: Use response-based titration rules (not just a calendar)
Here are practical rules I’ve used when helping people troubleshoot their retatrutide cagrilintide stacking schedule:
- If nausea or reflux increases: hold the current dose for an extra cycle (or longer) instead of escalating; reduce meal size and fat; prioritize hydration.
- If constipation worsens: do not “power through.” Adjust diet (fiber + water) and use a clinician-approved bowel plan; consider slowing titration.
- If appetite suppression becomes unmanageable: avoid forcing large meals. If you’re unintentionally under-eating, slowing titration usually improves both adherence and tolerability.
- If weight loss stalls early: first check adherence, protein intake, and constipation-related scale effects before increasing.
Example protocol timeline (structure)
This is a structure example to show how the ramp often gets staged. Your clinician should map the dosing amounts and intervals to your specific situation and the available formulations.
| Phase | Goal | Typical actions | What you monitor |
|---|---|---|---|
| Lead-in (Drug A) | Tolerability and baseline response | Start low, titrate gradually until side effects settle | Nausea, reflux, appetite control, bowel habits, hydration |
| Add Drug B | Maintain tolerability while gaining additive effect | Introduce second agent conservatively; slower escalation than Drug A | Same as above + energy level and meal size feasibility |
| Optimization | Find the “sweet spot” dose | Titrate only if side effects remain manageable | Weight trend (not day-to-day), waist measurement, adherence |
Side effects, troubleshooting, and when to pause
When combining therapies like retatrutide cagrilintide, troubleshooting isn’t optional—it’s part of the protocol. In real-world scenarios I’ve seen, the difference between “works” and “fails” is whether the dosing plan has clear pause rules.
Common issues and practical adjustments
- GI discomfort (nausea, reflux): smaller meals, avoid high-fat foods during titration, slow the ramp, consider clinician guidance for anti-nausea or reflux strategies.
- Constipation: hydration + fiber; add an approved bowel regimen; slow escalation if needed.
- Low energy from reduced intake: increase meal frequency (smaller portions), prioritize protein, and ensure you’re not under-hydrating.
Pause / reassess triggers
Pause and reassess with a clinician if you experience severe or persistent symptoms, signs of dehydration, intolerable inability to eat, or any concerning medical symptoms. A good stacking plan is designed to prevent escalation when your body is signaling it can’t tolerate the current combination.
Diet, protein, and adherence: the part most “stacks” ignore
Weight loss outcomes with retatrutide cagrilintide stacking depend heavily on adherence. The biggest adherence killers are under-eating, constipation, and meal timing that doesn’t match slowed gastric emptying.
My go-to nutrition structure during titration
- Protein first: aim for protein at every meal to preserve lean mass.
- Smaller, earlier meals: many people tolerate breakfast/lunch better than late-day heavy meals.
- Track bowel regularity: don’t wait for a full problem—use prevention.
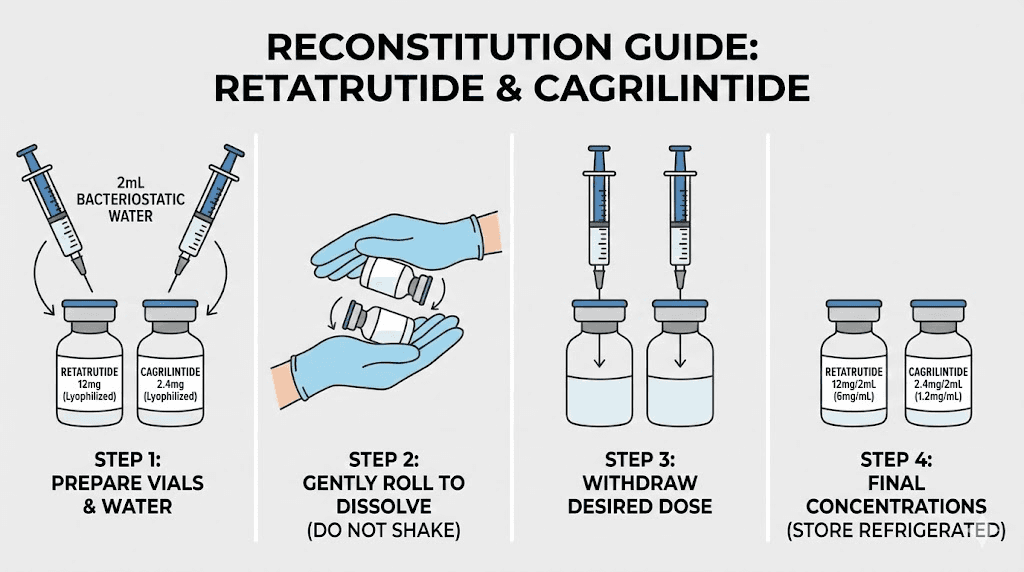
Image reference
FAQ
How do I decide which to start first for retatrutide cagrilintide stacking?
Clinicians often choose based on your baseline risk profile, tolerability, and the expected side-effect pattern. In my practical protocol reviews, the lead-in drug is usually the one you can titrate more comfortably first—because the real goal is to establish a tolerability baseline before adding the second agent.
What’s the safest way to speed up or slow down during the stack?
Use response-based rules: increase only when side effects stay mild and predictable. If GI symptoms or constipation worsen, hold longer at the current dose rather than escalating on schedule.
Will combining retatrutide cagrilintide always increase results?
It can, but it also increases the chance of intolerance. Additive effects aren’t guaranteed, and diminishing returns happen when tolerability limits adherence or when constipation-related scale changes mask true fat-loss progress.
Conclusion
A solid retatrutide cagrilintide stacking plan isn’t defined by a single dosing number—it’s defined by sequencing, titration pace, and response-based rules for side effects. In my hands-on experience, the most reliable improvements come from starting with a lead-in period, introducing the second agent conservatively, and using clear pause/hold decisions when GI or hydration issues show up.
Next step: Write down your current tolerability baseline (nausea level, reflux, bowel regularity, typical meal size) for the lead-in phase, then bring that snapshot to your clinician to finalize the sequencing and escalation rules for the full stack.
Discussion