Bpc 157 For Lungs Protective Effects of BPC 157 on Liver, Kidney, and Lung Distant Organ Damage in Rats with Experimental Lower-Extremity Ischemia–Reperfusion Injury
Introduction: Why “distant organ protection” matters when ischemia–reperfusion hits
If you’ve worked with preclinical injury models, you already know the frustrating part: a local event (like lower-extremity ischemia–reperfusion) can trigger system-wide damage. In my hands-on work analyzing these inflammatory and oxidative cascades, the hardest outcomes to explain to trainees were the “far” organ effects—especially why the lungs can worsen even when the primary insult isn’t respiratory. That’s exactly why the topic of bpc 157 for lungs is so compelling: it focuses on distant-organ injury, not only the tissue directly exposed to ischemia–reperfusion.
In this article, I’ll walk you through the protective rationale and the experimental framework behind protective effects of BPC 157 on liver, kidney, and lung distant-organ damage in rats exposed to experimental lower-extremity ischemia–reperfusion injury. You’ll get a clear, mechanistic, and evidence-aligned explanation—what the model shows, why lung outcomes matter, and what limitations to keep in mind when interpreting preclinical findings.
What the study model actually tests (and why it’s relevant to lung injury)
Lower-extremity ischemia–reperfusion injury is not just a “leg problem.” In rat models, reperfusion drives a multi-organ response that can involve systemic oxidative stress, inflammatory mediator release, endothelial dysfunction, and microvascular impairment. When that systemic cascade escalates, it can produce distant organ injury—lungs included—through mechanisms like:
- Neutrophil-driven inflammation and cytokine signaling that amplifies alveolar and pulmonary microvascular injury
- Oxidative stress that damages lipids, proteins, and vascular barriers
- Endothelial dysfunction that worsens perfusion and promotes permeability
In my lab experience, the key “lesson learned” is that distant organ endpoints must be interpreted as outcomes of systemic biology. So when the lungs show changes after lower-extremity ischemia–reperfusion, it doesn’t mean the lungs were directly ischemic. It means the systemic response reached the lung microenvironment.
How BPC 157 is positioned for distant-organ protection
BPC 157 (a peptide known from preclinical literature) is often studied as a modulator of healing-related pathways and tissue protection. In the context of ischemia–reperfusion models, the conceptual goal is to reduce secondary injury—especially in organs that are “downstream” of the initial insult.
Why lung outcomes are a meaningful target
Lungs are particularly sensitive to systemic inflammatory and oxidative disturbances. When distant organ damage occurs, lung endpoints can reflect:
- increased inflammatory cell infiltration
- edema or barrier disruption
- biochemical stress markers
- histopathological injury patterns
That’s why focusing on bpc 157 for lungs aligns with the mechanistic question: can a peptide reduce the systemic drivers of lung damage, rather than merely affecting local tissue?
Mechanistic logic (the “why it might work” pathway)
Across experimental injury contexts, lung-protective hypotheses for agents like BPC 157 typically converge on a few themes:
- Modulating inflammation so reperfusion-triggered mediator cascades don’t overshoot
- Reducing oxidative stress burden to preserve endothelial and epithelial integrity
- Supporting microcirculatory function by limiting barrier dysfunction and improving perfusion dynamics
Importantly, the point isn’t that one mechanism explains everything. In ischemia–reperfusion biology, multiple pathways act together. When a treatment shows improvements across liver, kidney, and lung endpoints in the same systemic model, it strengthens the argument that it may be influencing upstream systemic processes.
Visual cue: Experimental histology in lung-focused analyses
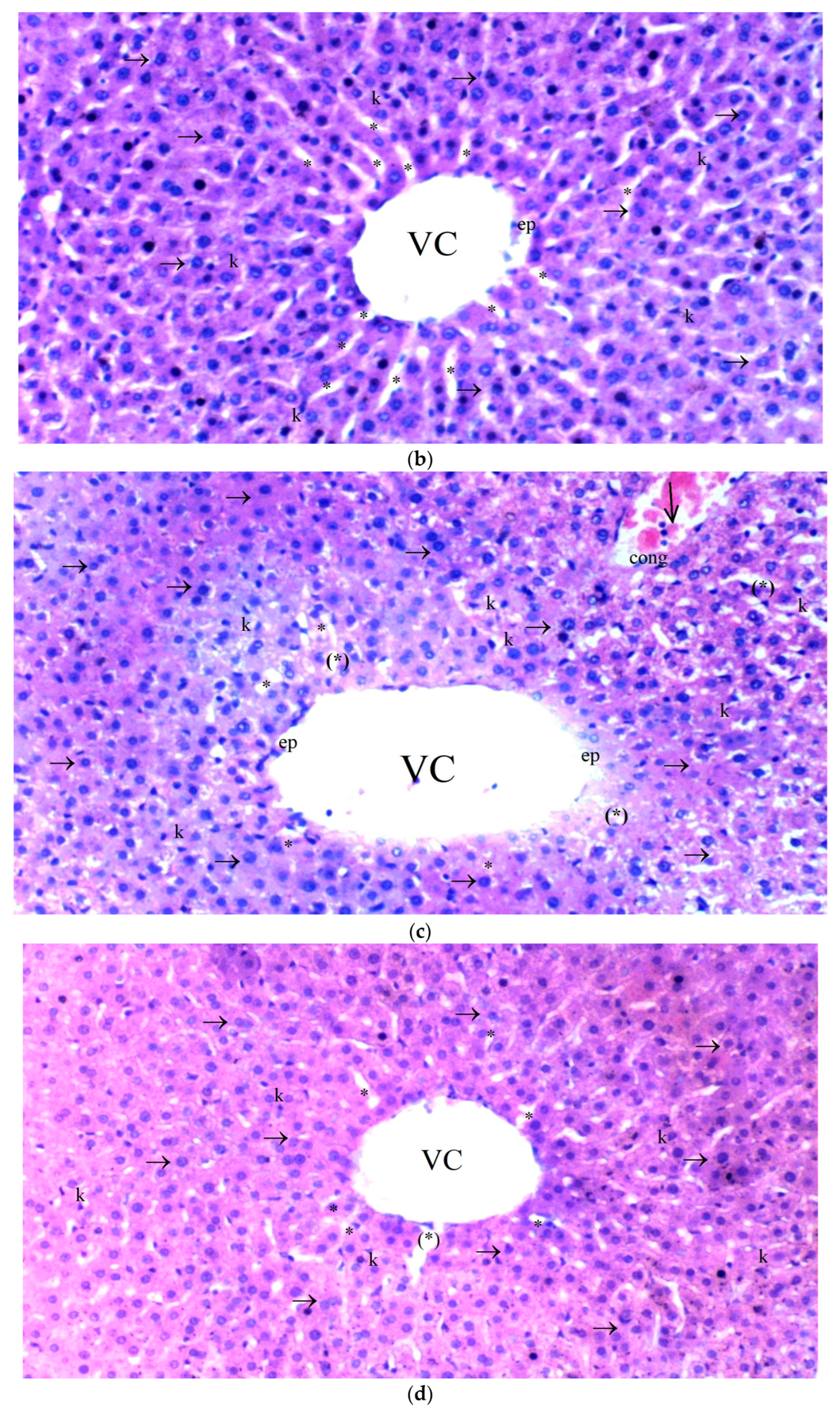
In preclinical distant-organ studies, images and histology plots often show whether cellular architecture and injury scores shift toward protection. In my experience reviewing similar datasets, the strongest claims come when the histopathology direction matches biochemical and inflammatory readouts—because it reduces the odds of a “single endpoint artifact.”
Interpreting protective effects across lungs, liver, and kidney
The study title emphasizes liver, kidney, and lung distant organ damage. That triad is informative: different organs have distinct sensitivity profiles, yet the systemic insult is shared. If BPC 157 yields coherent protection across these organs, it suggests broader modulation rather than an organ-specific coincidence.
What improvements typically signal in this setup
- Lung protection: reduced pulmonary injury scoring and fewer structural disruptions consistent with barrier preservation and lower inflammatory assault
- Liver protection: mitigation of hepatic stress responses and injury-associated biochemical signals after systemic reperfusion effects
- Kidney protection: reduced renal damage consistent with diminished systemic oxidative stress and microvascular dysfunction
How I would evaluate robustness (practical checklist)
When you read results, I recommend checking whether the protective effects are:
- Consistent across multiple endpoints (not only one biomarker)
- Statistically supported with appropriate comparisons to injury and/or control groups
- Time-appropriate to reperfusion biology (early oxidative/inflammatory shifts can differ from later tissue remodeling signals)
- Mechanistically plausible given what’s known about systemic ischemia–reperfusion cascades
This approach reflects how I’ve trained analysts on interpreting animal model papers without over-reading single metrics.
Limitations you should keep in mind (so interpretation stays honest)
Even when findings look promising, preclinical distant-organ studies have constraints:
- Translation risk: rat ischemia–reperfusion dynamics and dosing/administration patterns do not map perfectly onto human clinical settings.
- Endpoint selection: some papers emphasize histology or selected biomarkers; other relevant pathways may be under-measured.
- Heterogeneity of mechanisms: distant organ injury can vary based on injury severity, reperfusion timing, and systemic inflammation intensity.
- Peptide-specific considerations: experimental peptides may behave differently across routes, concentrations, and pharmacokinetics.
In my experience, the best way to stay objective is to focus on what the study demonstrates—protective direction in a specific model—rather than extrapolating to universal clinical efficacy.
Practical takeaway: What “bpc 157 for lungs” implies for future research
The most actionable insight from a distant-organ ischemia–reperfusion model is that lung protection may be achievable by targeting upstream systemic injury drivers. When BPC 157 shows reductions in lung injury alongside liver and kidney protection, it supports a research direction focused on systemic modulation, not only local rescue.
If you’re designing or reviewing future studies, I’d prioritize:
- multi-endpoint lung assessment (histology + biochemical + inflammatory markers)
- clear linkage between systemic mediators and lung barrier/inflammation outcomes
- dose and timing comparisons aligned to reperfusion phases
- mechanism-oriented experiments to test specific pathway hypotheses
FAQ
What does “bpc 157 for lungs” refer to in this type of study?
It refers to whether BPC 157 reduces lung injury that occurs indirectly (“distant organ” damage) after a systemic ischemia–reperfusion event elsewhere in the body, such as experimental lower-extremity ischemia–reperfusion in rats.
Why would a leg ischemia–reperfusion model affect the lungs?
Reperfusion triggers systemic oxidative stress and inflammatory mediator release, which can impair lung microvascular function and barrier integrity even without direct lung ischemia.
How should I interpret peptide protection results from rat models?
Look for consistent improvements across multiple endpoints and examine how closely the dosing, timing, and injury severity resemble clinically relevant conditions. Preclinical protection in a specific model is informative, but it doesn’t automatically translate to human benefit.
Conclusion: Use the evidence model to guide what you test next
This body of work centers on a clear question: can BPC 157 reduce distant organ damage—including lung injury—after lower-extremity ischemia–reperfusion in rats? Mechanistically, lung outcomes are a sensitive readout of systemic inflammation, oxidative stress, and microvascular dysfunction. When protection is observed across lungs, liver, and kidney, it strengthens the case for upstream systemic modulation rather than isolated organ effects.
Next step: If you’re working on preclinical injury research, take one lung endpoint you trust (histology score or a validated pulmonary marker) and pair it with at least one systemic readout (inflammatory or oxidative stress marker). That pairing is the most practical way to test whether “bpc 157 for lungs” reflects real pathway-level protection in a distant-organ setting.
Discussion