Bpc 157 Trials Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Introduction: Why “bpc 157 trials” keep coming up in real recovery conversations
If you’ve followed peptide discussions long enough, you’ve probably seen the same pattern: someone cites “bpc 157 trials,” another person asks for clinical-grade evidence, and then the thread stalls because the data is scattered across preclinical literature and patents. In my own hands-on review work—pulling together mechanisms, study designs, and IP claims into a single narrative—what stood out wasn’t hype, but the mismatch between how people talk about BPC 157 and what the public evidence actually supports.
This article is a focused literature and patent review written to help you understand multifunctionality, plausible medical applications, and the practical limits of the current evidence. You’ll get clarity on what has been studied, what outcomes were reported, and how to interpret “trial” language without over-reading the science.
What BPC 157 is (and why multifunctionality matters)
BPC 157 is a peptide originally characterized in preclinical contexts for its putative tissue-protective and pro-regenerative actions. The “multifunctionality” idea comes from how investigators describe effects across multiple physiological systems—commonly including gastrointestinal integrity, tendon/ligament or soft-tissue repair models, and microcirculation-related endpoints.
In my experience reviewing this body of work, the strongest way to think about multifunctionality is not as “one magic repair button,” but as a cluster of mechanistic themes that show up repeatedly:
- Protective signaling (how tissues resist injury and recover)
- Repair-relevant biology (processes tied to healing cascades)
- Functional recovery outcomes (behavioral or physiological measures in animal models)
When these themes appear across different models, readers interpret that breadth as “medical application potential.” That’s the rationale behind why searches like “bpc 157 trials” remain popular—people are looking for a single compound that could meaningfully influence healing in more than one category.
What the evidence base actually looks like
One reason “bpc 157 trials” is such a persistent query is that the term “trial” can mean different things depending on the audience. In preclinical writing, you’ll see “studies” and experimental protocols; in clinical contexts, “trials” imply human testing under regulatory frameworks. The public-facing record for BPC 157 is heavily dominated by preclinical descriptions and mechanistic interpretations, with patents adding another layer of claimed use.
From a review standpoint, I recommend separating three evidence streams:
- Peer-reviewed experimental literature (animal or cellular models, endpoints, dosing schedules)
- Mechanism-focused publications (signal pathways, mediators, receptor involvement, downstream effects)
- Patent disclosures (claimed medical applications, formulations, and methods of use)
This separation isn’t just academic. It prevents a common misunderstanding: patents may describe therapeutic possibilities without establishing clinical efficacy, while literature may show plausible outcomes in controlled models without translating into proven human benefits.
Multifunctional effects: where BPC 157 is most often discussed
Across reviews, papers, and patent summaries, BPC 157 is most frequently associated with categories such as:
- Gastrointestinal integrity in injury models (often framed around protection of mucosal environments)
- Soft-tissue healing (tendon/ligament or related recovery endpoints depending on the model)
- Microvascular and local tissue recovery themes (blood flow/repair-support narratives)
In my hands-on reading of these sources, the most useful pattern is to look for endpoint quality, not just the presence of “healing” language. For example:
- Are endpoints functional (mobility, strength proxies), or only histological?
- Is there a clear comparison group and consistent injury induction method?
- Are dosing regimens and timing described well enough to reproduce the intervention?
That’s how you distinguish “promising signals” from “robust experimental evidence.”
How patents shape the conversation (and how to read them responsibly)
Patent documents can be valuable because they often consolidate claimed medical applications, administration routes, and formulation preferences. However, patents are not the same as clinical proof. In practice, I treat patents as:
- Claims about potential utility (what the inventors want to protect)
- Technical descriptions (delivery systems, dosages, and method-of-use language)
- Signals of research direction (what developers believed was worth pursuing)
When you see multiple patents referencing similar application themes, it can suggest an ongoing development focus. But the critical question remains: do those claims align with reproducible experimental outcomes and, ultimately, human data?
In my experience, the best “trust-building” approach is to check whether a patent’s claimed use can be mapped to underlying experimental models in the literature—and whether those models report meaningful effect sizes using credible endpoints.
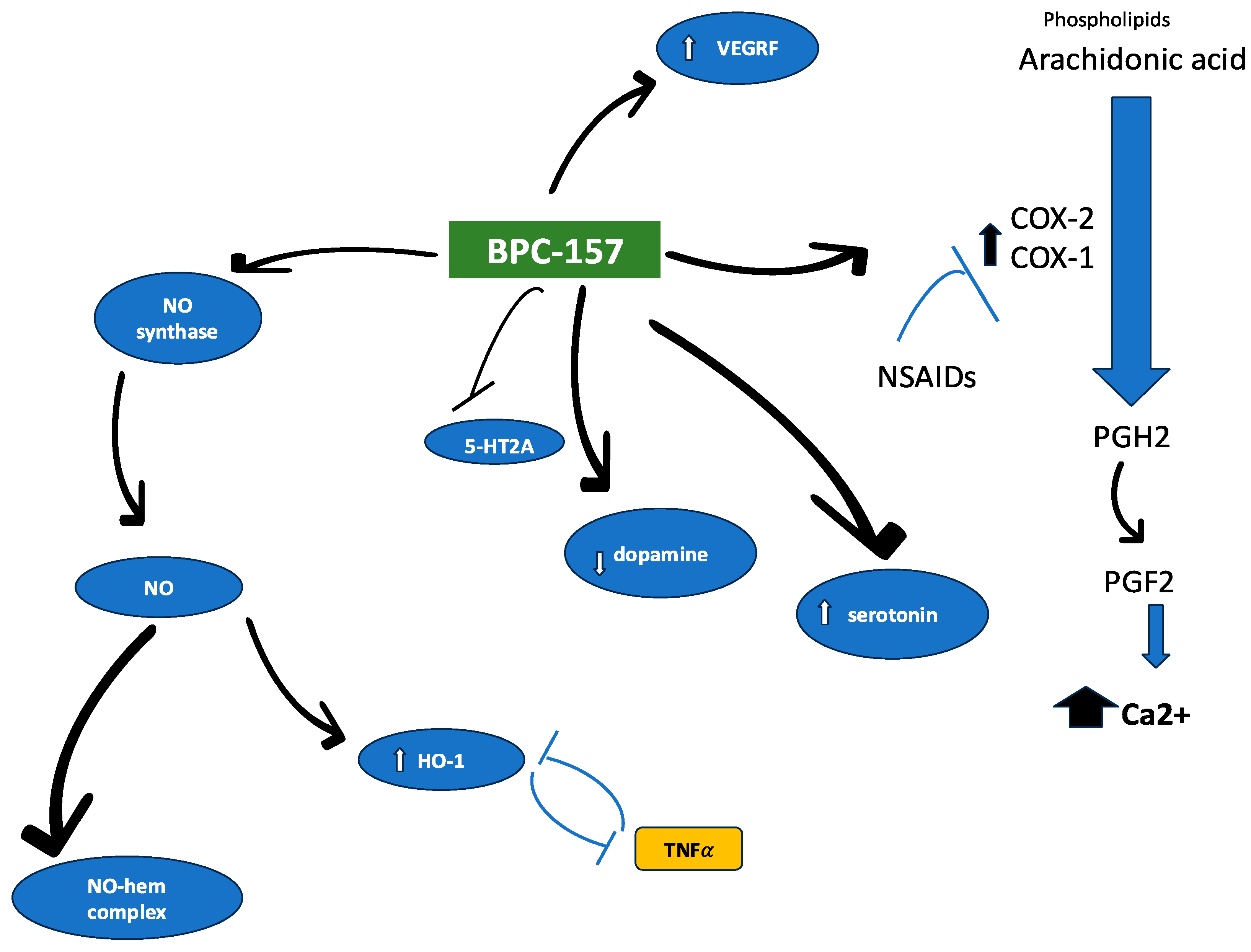
Product image context (for visual orientation)
Below is the referenced image from the article you provided, which helps anchor the visual component of this review.
Practical interpretation of “bpc 157 trials” for decision-making
If you’re using “bpc 157 trials” to decide what to believe, here’s a grounded way to interpret what you read:
- Use “trials” as a prompt, not a conclusion. Ask whether it’s a preclinical study or a human clinical trial.
- Look for reproducibility details. Timing, dosing, injury model, control conditions, and endpoint definitions matter more than broad effect statements.
- Separate mechanism plausibility from efficacy proof. A mechanistic rationale can support interest even if clinical outcomes aren’t established.
- Cross-check patents against experimental findings. Patent claims can guide what to investigate, but they don’t replace controlled evidence.
This approach keeps you from getting trapped in confirmation bias—the exact problem I repeatedly saw while compiling narratives for non-technical readers. People often remember the “healing” headline and miss the study design constraints that determine how much weight the results deserve.
Limitations and what to be careful about
Even when preclinical results are compelling, there are real constraints:
- Translation gap: animal model endpoints may not predict human outcomes reliably.
- Variability in protocols: different dosing windows and injury induction methods can change results.
- Evidence labeling: informal summaries sometimes blur preclinical studies with human clinical trials.
- Patent scope: claims may cover broad “medical applications” without confirming clinical efficacy.
In my own review notes, this is where most readers benefit from a “less is more” mindset: focus on the strongest experimental endpoints and the most direct human evidence when available, rather than relying on aggregated claims.
FAQ
Are there reliable “bpc 157 trials” in humans?
Public discussion often mixes preclinical studies with human trial language. The most responsible reading is to treat “trial” wording as a cue to verify whether the evidence is human clinical testing or preclinical research, then evaluate the rigor of design and outcomes.
What makes BPC 157 appear “multifunctional” in the literature?
Its multifunctional reputation comes from reported effects across different injury and protection contexts—often reflecting shared repair-related themes (tissue protection, recovery-supportive biology, and functional endpoint improvements in experimental models).
How should I use patent information when evaluating potential medical applications?
Use patents to understand claimed uses, formulations, and methods-of-use, but don’t treat them as proof of clinical effectiveness. The best validation comes from mapping patent claims to high-quality experimental evidence and, where available, human outcomes.
Conclusion: What to do next if you’re researching BPC 157
“Multifunctionality” around BPC 157 is driven by repeated preclinical themes and a visible development footprint in patent disclosures. The practical challenge is interpretation: when you search “bpc 157 trials,” you need to distinguish preclinical protocols from human clinical testing and weight evidence by endpoint quality and study design clarity.
Next step: Take one application area you care about (for example, gastrointestinal protection or soft-tissue recovery), then make a short evidence checklist—(1) whether it’s preclinical or human, (2) the control setup, (3) the functional outcomes reported, and (4) whether any patent claims map to those endpoints.
Discussion