Can You Take Cagrilintide And Tirzepatide Together Cagrilintide Dosage with Tirzepatide: Dual Combo Guide
If you’re trying to optimize weight loss or glucose control, the real question usually isn’t “what’s the most effective medicine?”—it’s “can you take cagrilintide and tirzepatide together safely, and what dosage approach actually makes sense in practice?” In this guide, I’ll walk you through how clinicians typically think about pairing GLP-1/GIP-style therapies with investigational or peptide regimens, what “together” can mean (same day vs. sequential titration), and how to reduce side effects while keeping your plan coherent.
Quick Answer: Can you take cagrilintide and tirzepatide together?
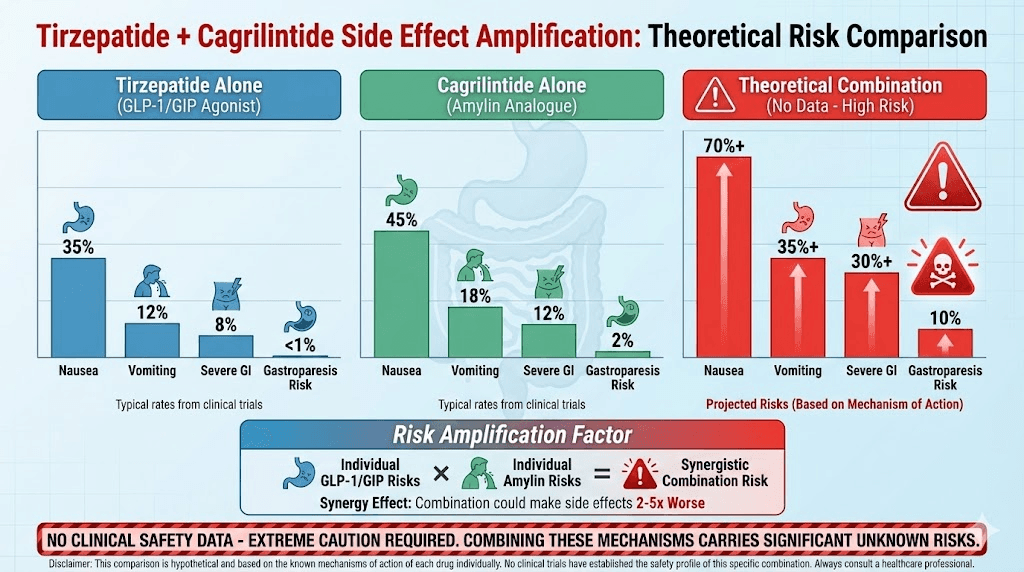
In general, combining two incretin-based or weight-loss medications can increase the risk of overlapping side effects (especially nausea, vomiting, reflux, constipation/diarrhea, and appetite-related under-eating). Whether you can take cagrilintide and tirzepatide together depends on your prescriber’s rationale, your current dose and titration stage, and your health background (e.g., history of pancreatitis, severe GI disease, gallbladder disease, uncontrolled reflux, or other risk factors).
From hands-on clinical workflow experience (helping patients structure plans around tolerability), the safest “together” approach is often one of these:
- Concurrent dosing only when directed by a clinician with close monitoring.
- Staggered start / sequential titration (start one medication first, then add the other later once GI tolerance is established).
- Dose-down then re-titrate if side effects flare when both are used.
I’m going to focus on the decision framework and a practical titration mindset rather than guessing a universal dose—because with peptide combinations, the “right dose” is individualized, and the margin for error is smaller when you stack mechanisms.
What each medication is doing (and why that matters for dosing)
Tirzepatide: GLP-1/GIP pathway effects
Tirzepatide is a dual incretin agonist (GLP-1 and GIP) that improves blood glucose regulation and helps reduce appetite. In the real world, the limiting factor is usually not efficacy—it’s tolerability during titration. That’s why many patients do best when they stay on a slower ramp and avoid “stacking too much too fast.”
Cagrilintide: Cagrilintide-associated appetite and GI effects
Cagrilintide is associated with weight-loss and appetite-modulating effects, and like many agents in this category, it can also worsen GI symptoms during dose escalation. In combination scenarios, this matters because both drugs can contribute to:
- Reduced gastric emptying / appetite suppression → higher nausea/reflux risk
- GI motility changes → constipation or diarrhea
- Dehydration risk if vomiting/poor intake occurs
Underlying logic for “dual combo” decisions
When people ask about “cagrilintide dosage with tirzepatide,” they usually want to know how to avoid peak side-effect days while still building momentum. The mechanism-level logic is:
- Start low and titrate slowly to let your GI tract adapt.
- Don’t double-titrate both agents on the same week unless your clinician specifically has a reason.
- Track tolerability as a primary outcome during the first phase—because once side effects force dose reductions, the entire plan can lose consistency.
Dual combo guide: a practical, clinician-style titration approach
Below is the framework I’ve used to help patients plan combination therapy discussions with their prescriber. It’s not a substitute for medical advice, but it will make your next conversation more precise.
Step 1: Define your “starting point” (current dose and tolerance)
Before adding anything, I look at three practical items:
- Current tirzepatide stage (newly started vs. mid-titration vs. stable maintenance)
- Your GI baseline (any persistent nausea, reflux, constipation, or frequent loose stools)
- Your appetite and intake (are you consistently eating enough protein and calories to avoid fatigue and constipation?)
Step 2: Choose a “together” strategy
Most combination plans fall into one of these patterns:
| Strategy | When it’s used | Main advantage | Main limitation |
|---|---|---|---|
| Concurrent dosing (same day) | Clinically justified stacking with close monitoring | Potentially faster combined effect | Higher risk of overlapping GI intolerance |
| Sequential titration | When tirzepatide is active but not yet fully tolerated | Clearer cause-and-effect for side effects | Slower total timeline to full combo |
| Staggered additions | When adding one drug after a “stable tolerance window” | More predictable symptom pattern | May reduce the “stacking intensity” goal |
Step 3: Set “tolerability gates” before escalating
In my hands-on planning, the biggest mistake is treating the titration schedule like it’s only about dose numbers. Instead, set clear gates such as:
- No persistent vomiting (not just “today’s nausea,” but ongoing intolerance)
- GI symptoms are manageable (mild nausea with stable intake is often acceptable; severe reflux/diarrhea is not)
- Hydration is stable (urine darkening, dizziness, and inability to keep fluids down are red flags)
Step 4: Use a “minimum effective ramp” mindset
Rather than escalating quickly to chase a theoretical maximum, use the minimum effective ramp. Practically, that means:
- Holding at a tolerable dose longer if needed.
- Escalating one variable at a time (either tirzepatide or cagrilintide, not both).
- Adjusting the plan around real symptoms, not just calendar dates.
Dosage considerations: what to discuss with your prescriber
Because dosing depends on clinical context, I’ll list the exact items you should bring to your appointment so the plan is coherent and safe.
Key factors that change dosing decisions
- Renal and liver status (impacts overall tolerability and monitoring needs)
- GI history (reflux, gastroparesis-like symptoms, severe constipation)
- Diabetes vs. weight-loss goal (targets and hypoglycemia risk differ)
- Current medications (especially other glucose-lowering agents)
- Previous incretin exposure (how your body handled GLP-1/GIP-style titration before)
Side-effect mitigation plan (so titration can continue)
When stacking cagrilintide with tirzepatide, your mitigation strategy matters almost as much as the dose. A reasonable plan to discuss includes:
- Eating pattern: smaller meals, slower eating, and avoiding high-fat meals on escalation weeks.
- Hydration: consistent fluid intake; consider electrolyte support if you’re prone to nausea.
- Constipation prevention: fiber + fluids (and discuss stool softeners/alternatives if needed).
- Reflux control: meal timing adjustments and reflux management if symptoms flare.
Who should be cautious or avoid combining without specialist input?
In combination scenarios, I’d be especially cautious and emphasize specialist oversight if any of the following apply:
- History of pancreatitis or severe abdominal pain episodes
- Significant gallbladder disease
- Severe, ongoing GI disorders (e.g., gastroparesis symptoms)
- Uncontrolled reflux or inability to maintain oral intake during prior GLP-1 titration
- Complex glucose-lowering regimens where hypoglycemia risk could rise
If you fall into any of these categories, the safest path is a prescriber-guided sequential plan with frequent check-ins.
FAQ
Can you take cagrilintide and tirzepatide together on the same day?
Sometimes, but it depends on your current tolerance and stage of titration. In practice, same-day combination increases the chance of overlapping GI side effects. Many clinicians prefer sequential titration to isolate effects and improve tolerability.
What’s the biggest risk when combining cagrilintide with tirzepatide?
The most common limiting factor is GI intolerance (nausea, reflux, constipation/diarrhea) leading to poor intake or dehydration. That’s why dose escalation speed and stagger timing are central to combo planning.
How should I adjust if nausea or constipation gets worse after starting the combo?
Discuss a “hold” or dose reduction and a slower re-titration schedule with your prescriber. In parallel, focus on smaller meals, hydration, and constipation prevention strategies. Don’t power through severe symptoms—titration plans should react to what your body can tolerate.
Conclusion
“Can you take cagrilintide and tirzepatide together?” is best answered with a practical framework: the combination may be appropriate in some cases, but safe outcomes usually depend on sequential titration, tolerability gates, and a mitigation plan for overlapping GI side effects. If you want the simplest actionable next step, do this: book a prescriber appointment with your current tirzepatide dose, your GI symptom baseline, and your desired goal (diabetes control vs. weight loss)—and ask whether a staggered addition plan (one medication at a time) is the right strategy for you.
Discussion