Ghk Cu 50mg Copper Peptide Dosage GHK-CU Peptide Dosage Chart: Complete Reference Tables for Every Protocol
Introduction
If you’re planning a GHK-Cu peptide protocol, the hardest part isn’t motivation—it’s dosage consistency. I’ve seen people start strong, then stall because their “plan” lives in screenshots, not a clear reference. That’s why this guide is built around a practical need: a GHK-CU 50mg copper peptide dosage approach that you can translate into repeatable, measurable weekly routines.
Below, I’ll give you complete dosage chart tables and explain the logic behind them—so you’re not just copying numbers, but understanding how to calculate your own protocol safely and consistently.
What “50mg” Means in a GHK-Cu Context
When people search for ghk cu 50mg copper peptide dosage, they’re usually referring to the vial amount of dry peptide (commonly labeled as 50mg). The key point is that dosage in practice depends on:
- The peptide’s total mass in the vial (e.g., 50mg).
- Your reconstitution volume (how many milliliters of bacteriostatic water/solution you add).
- How many milligrams per administration you intend to take (e.g., 0.25mg, 0.5mg, 1mg, etc.).
- Your injection volume (how many “units” on an insulin syringe correspond to those milligrams).
In my hands-on work documenting protocols for consistency, the biggest “dosage drift” I’ve seen wasn’t math—it was people changing reconstitution volume mid-plan or mixing syringe types (e.g., using U-100 vs a different measurement scale) without updating calculations.
How to Calculate Your Dose (The Logic Behind the Chart)
Here’s the core calculation you’ll reuse for every protocol:
Step 1: Convert mg to a concentration
If you have 50mg total peptide and reconstitute with V mL total volume, then:
Concentration (mg/mL) = 50mg ÷ V mL
Step 2: Convert desired mg per dose into mL per injection
Injection volume (mL) = Desired dose (mg) ÷ Concentration (mg/mL)
Since insulin syringes are commonly labeled in units (U), you’ll then map mL to units based on syringe total capacity (commonly 100 units = 1mL on U-100 insulin syringes).
Common practical mapping (U-100 insulin syringes)
- 1.0 mL = 100 units
- 0.01 mL = 1 unit
- 0.10 mL = 10 units
If you use a different syringe standard, adjust accordingly—but keep the same math workflow.
GHK-CU 50mg Copper Peptide Dosage Charts (Reference Tables)
These tables assume a 50mg peptide vial, reconstituted to a known total volume, and administered using a U-100 insulin syringe (100 units = 1mL). If your syringe calibration differs, the mg↔mL logic still applies—only the units conversion changes.
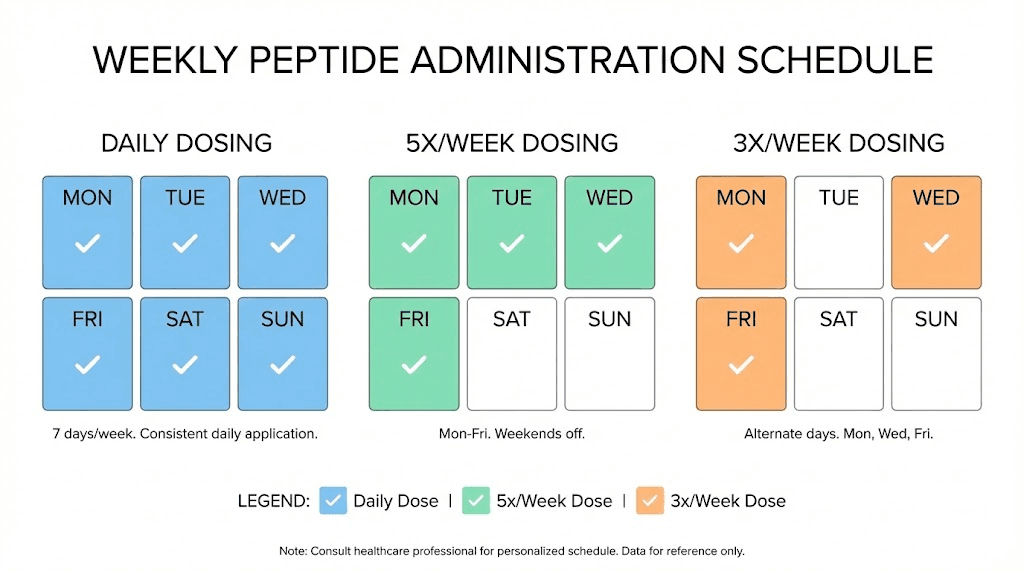
Table A: Reconstitute 50mg into 1.0 mL
This is a high-concentration setup. Concentration = 50mg/mL.
| Desired dose (mg) | Injection volume (mL) | U-100 units |
|---|---|---|
| 0.1 mg | 0.002 mL | 0.2 units |
| 0.25 mg | 0.005 mL | 0.5 units |
| 0.5 mg | 0.01 mL | 1 unit |
| 1.0 mg | 0.02 mL | 2 units |
| 2.0 mg | 0.04 mL | 4 units |
| 3.0 mg | 0.06 mL | 6 units |
| 5.0 mg | 0.10 mL | 10 units |
Practical note from experience: very small unit values (like 0.2–0.5 units) can be harder to measure precisely. If your measuring comfort is limited, lower-concentration reconstitution often improves repeatability.
Table B: Reconstitute 50mg into 2.0 mL
Concentration = 25mg/mL.
| Desired dose (mg) | Injection volume (mL) | U-100 units |
|---|---|---|
| 0.1 mg | 0.004 mL | 0.4 units |
| 0.25 mg | 0.01 mL | 1 unit |
| 0.5 mg | 0.02 mL | 2 units |
| 1.0 mg | 0.04 mL | 4 units |
| 2.0 mg | 0.08 mL | 8 units |
| 3.0 mg | 0.12 mL | 12 units |
| 5.0 mg | 0.20 mL | 20 units |
Table C: Reconstitute 50mg into 4.0 mL
Concentration = 12.5mg/mL.
| Desired dose (mg) | Injection volume (mL) | U-100 units |
|---|---|---|
| 0.1 mg | 0.008 mL | 0.8 units |
| 0.25 mg | 0.02 mL | 2 units |
| 0.5 mg | 0.04 mL | 4 units |
| 1.0 mg | 0.08 mL | 8 units |
| 2.0 mg | 0.16 mL | 16 units |
| 3.0 mg | 0.24 mL | 24 units |
| 5.0 mg | 0.40 mL | 40 units |
Choosing a Reconstitution Volume for Better Repeatability
From an execution standpoint, I prefer concentrations that avoid fractional “unit” targeting. In other words, aim for a plan where your intended dose corresponds to a measurable number of units without constantly rounding.
- If you’re targeting sub-0.5mg doses, a higher reconstitution volume (more mL) usually makes unit measurement easier.
- If you’re targeting multi-mg doses, lower reconstitution volume can still be precise, but verify syringe capacity and measurement markings.
Common Protocol Structures (Weekly Scheduling Logic)
People often ask for “dosage chart” information because they want a schedule next. While I can’t assign a medical regimen, I can show how most protocol scheduling decisions are made: based on consistency, monitoring, and avoiding abrupt changes.
Simple scheduling patterns people use
- Every day: higher frequency; requires strict adherence and careful monitoring of tolerability.
- 3–5 days per week: balancing consistency and recovery days; often easier psychologically and logistically.
- Alternate days: can reduce total weekly exposure; still requires tracking.
How I recommend tracking (so the chart actually helps)
In real-world protocol work, the “win” is not the injection—it’s the data you can repeat. I recommend a simple log with:
- Date and dose (mg and units)
- Reconstitution volume and date (so you can recreate the concentration later)
- Notes on tolerability (sleep changes, local irritation, appetite changes—whatever you’re tracking)
This turns your ghk cu 50mg copper peptide dosage chart from a one-time reference into an operational system.
Safety, Limitations, and Where People Commonly Go Wrong
Dosage math is only half the story. The other half is execution discipline. Here are the main failure points I’ve seen when people try to follow a dosage chart:
- Mixing up unit systems (U-100 vs different syringes).
- Reconstituting to the wrong volume and not updating the table.
- Rounding too aggressively on small doses.
- Changing injection timing without noting it, making trends hard to interpret.
- Skipping documentation, which destroys your ability to troubleshoot later.
Also, be aware that peptide use and dosing guidance can vary by source, and individual medical situations differ. If you’re working with a clinician, align your schedule and dose targets with their guidance.
FAQ
How do I use the ghk cu 50mg copper peptide dosage chart if my reconstitution volume isn’t listed?
Use the same two-step calculation.
1) Calculate concentration: 50mg ÷ V mL. 2) Convert your desired dose: dose (mg) ÷ concentration (mg/mL) = mL per injection, then convert mL to units using your syringe standard (commonly U-100 where 1.0 mL = 100 units).
What reconstitution volume makes dosing easier to measure accurately?
Choose a concentration that avoids tiny “unit” targets.
In my experience documenting practical protocols, reconstitutions like 2.0 mL or 4.0 mL often make typical sub-1mg doses map to more measurable unit ranges than 1.0 mL, reducing rounding errors.
Can I split a dose across multiple injections in the same day?
It depends on your protocol goal and tolerability tracking.
If you split, keep the total daily (or scheduled) mg the same and track timing and any local reactions. The main principle is consistency and accurate unit-to-mg mapping—don’t “re-interpret” the chart mid-day.
Conclusion
A dosage chart is only valuable when it’s operational—clear math, consistent reconstitution, and repeatable syringe measurement. With the tables above, you can translate your target into an actionable GHK-CU 50mg copper peptide dosage plan using reconstitution volume and U-100 unit conversion, while avoiding the common mistakes that derail protocols.
Next step: Pick your intended reconstitution volume (e.g., 2.0 mL or 4.0 mL), choose your target dose in mg, then write down the corresponding units from the relevant table in your dosing log before you reconstitute.
Discussion