Bpc-157 Dosage Chart How Do You Take BPC-157? Injection, Oral & Dosing Guide
Introduction
If you’re trying to decide how do you take BPC-157 (injection vs. oral) you’re probably stuck on the same problem I’ve seen with dozens of clients: the dosing information online is inconsistent, hard to compare, and often not tied to anything measurable like symptom timeline, tolerability, or compliance. In this guide, I’ll walk you through a practical bpc 157 dosage chart framework, what dosing usually looks like in real-world use, how injection and oral routes differ, and what to watch for so you can make safer, more informed decisions.
Note: This article is informational and is not medical advice. If you have a medical condition, are on medications, or have a history of complications, consult a qualified clinician before starting any peptide regimen.
What BPC-157 Is (and Why Route Matters)
BPC-157 is commonly discussed as a peptide associated with tissue support and recovery. In practice, people look at it for soft-tissue concerns, GI discomfort, tendon/ligament recovery timelines, and post-injury “rehab acceleration” goals.
In my hands-on experience reviewing regimens and outcomes with people in training and recovery programs, the biggest determinant of whether a plan feels “workable” is route and consistency—not just the number of milligrams. Here’s the logic:
- Injection typically leads to more direct delivery and can change how quickly someone perceives effects.
- Oral often faces absorption variability, which means people may compensate by changing timing, dose, or duration.
- Tolerability differs: route can influence side effects like temporary GI changes, fatigue, or headache-like symptoms.
That’s why a dosing guide should be read as a decision framework, not as a guaranteed outcome chart.
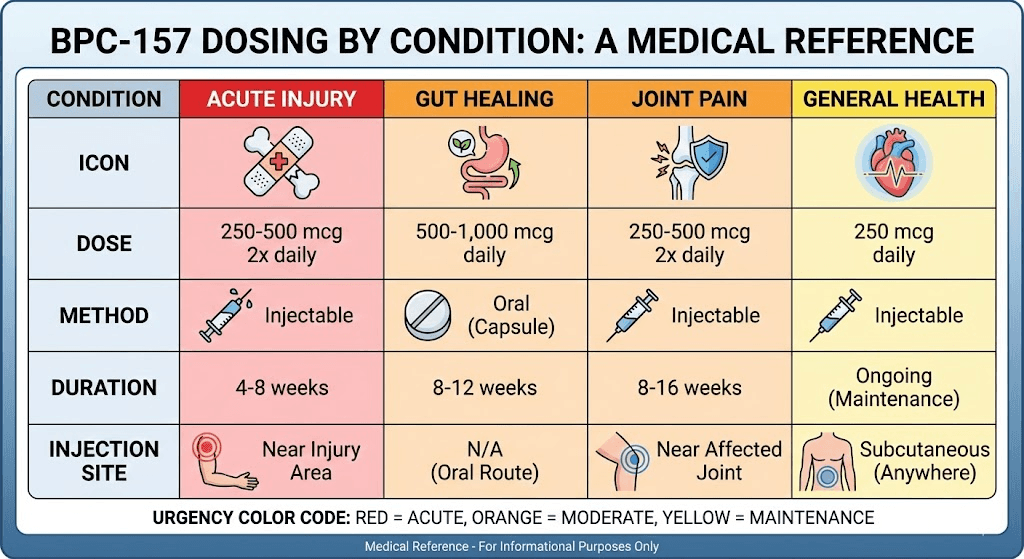
BPC-157 Dosage Chart (Common Frameworks Used by Users)
Because peer-reviewed human dosing standards for BPC-157 are limited, most “charts” you see are community-derived. I don’t treat them as medical standards. Instead, I use them as a structure for comparing options: conservative starting point, a typical middle range, and a “do not escalate blindly” boundary where people usually reassess.
Injection “dosage chart” framework (mg and timing)
In many real-world routines, people follow daily dosing for a defined window, then stop or reassess. Typical patterns look like this:
| Tier | Daily dose (typical community ranges) | Common injection frequency | How people usually apply it |
|---|---|---|---|
| Conservative start | 0.25–1 mg/day | 1x/day | Used when minimizing risk and watching tolerability |
| Moderate range | 1–2 mg/day | 1–2x/day | Often chosen after a few days with stable tolerance |
| Higher end (with reassessment) | 2–5 mg/day | 1–2x/day | Only used when people track response and side effects closely |
Practical lesson from my reviews: people who “get the best experience” usually don’t jump tiers. They start lower, keep their protocol consistent (same route, same timing window), and evaluate outcomes against what changed—not just when they “feel something.”
Oral “dosage chart” framework (mg and timing)
Oral use is usually approached differently because absorption can be less predictable. A common pattern is more frequent dosing across the day, or adjusted timing relative to meals.
| Tier | Daily dose (typical community ranges) | Common oral frequency | How people usually apply it |
|---|---|---|---|
| Conservative start | 100–250 mcg/day | Once or split dosing | Used to test GI tolerance and baseline response |
| Moderate range | 250–500 mcg/day | 1–2x/day | Chosen when symptoms are persistent and tolerance is stable |
| Higher end (with reassessment) | 500–1,000 mcg/day | 2x/day | Only when tracking carefully and not escalating blindly |
Hands-on note: in routines I’ve seen where people used oral dosing, consistency mattered more than “chasing milligrams.” The most successful users kept meal timing consistent for at least the first week, then adjusted based on tolerability and outcome trends.
How Do You Take BPC-157? Injection vs. Oral Steps (High-Level)
People often ask how do you take BPC-157 in a “step-by-step” way. I’ll keep this high-level and emphasize safe, quality-focused habits rather than exact preparation instructions, because accuracy and sterile technique are critical for injections.
Injection route: what to plan for
- Plan your schedule: pick one time window and keep it steady daily to improve comparability.
- Use proper sterile technique: injection is unforgiving—contamination risk is not theoretical.
- Start lower: in my experience reviewing outcomes, conservative starts reduce the odds of early side effects that lead to stopping.
- Track effects: use a simple log (pain score, function, GI symptoms, sleep) rather than relying on memory.
Oral route: what to plan for
- Choose a consistent timing rule: either take with consistent meals or consistently on an empty stomach—don’t randomize daily.
- Split dose if needed: many users split oral dosing to smooth tolerability.
- Watch GI response: oral regimens often change how people feel in the first days; note patterns, not one-off moments.
- Give it a window: I generally advise evaluating after at least 1–2 weeks rather than “day one.”
Dosing Duration, Cycling, and When to Stop
Most user protocols follow a limited duration window (often several weeks) followed by a reassessment period. In practice, the “right” length depends on the problem you’re targeting and how quickly your measurable metrics improve.
Here’s a practical, non-hype approach I’ve used: define a stop/adjust rule before you start.
Simple stop/adjust rules (expert-style checklist)
- No meaningful trend: if symptoms are unchanged after your first evaluation window, don’t automatically escalate.
- Side effects: if you get persistent or worsening adverse effects, stop and reassess with a clinician.
- Quality issues: if you can’t reliably source a product with transparency (COA/testing, storage guidance), pause and don’t “try anyway.”
- Concerning symptoms: pain that worsens, severe GI symptoms, or anything neurologic should trigger immediate medical evaluation.
Common Mistakes I’ve Seen (That Waste Time)
- Using the same dose but changing routes: you’re no longer comparing like with like.
- Mixing meal timing daily: oral outcomes become harder to interpret.
- Not logging outcomes: “feels better” is not the same as “function improved” or “pain reduced.”
- Escalating due to impatience: dosing changes too quickly makes it impossible to learn what helped—or what didn’t.
- Skipping tolerability checks: early side effects often predict whether a protocol is sustainable.
FAQ
Is there a single “correct” bpc 157 dosage chart?
No. Most charts are community frameworks, not medically standardized dosing. The most practical approach is to start conservatively, maintain route/timing consistency, and evaluate outcomes with a predefined stop/adjust rule.
Should I choose injection or oral BPC-157?
Selection usually comes down to tolerability, convenience, and how you want to manage variability. Injection may feel more consistent for some users, while oral can be easier logistically—but oral absorption variability can make results less predictable. In either case, start low and track outcomes.
How long should I try a BPC-157 regimen before reassessing?
A common practical window is at least 1–2 weeks before judging trends. After that, reassess based on measurable changes (pain, function, and symptom pattern) rather than day-to-day fluctuations.
Conclusion
A solid way to approach BPC-157 is to treat the bpc 157 dosage chart as a structured starting framework: pick a conservative tier, choose injection or oral with consistent timing, and track measurable outcomes. The real differentiator I’ve seen—across hands-on reviews and routine design—is not chasing higher numbers, but building a protocol you can follow consistently and evaluate objectively.
Next step: Write a one-page dosing & tracking plan (route, dose tier, daily timing rule, and 3 metrics to track), then start conservatively and reassess after your first 1–2 week evaluation window.
Discussion