Cagrilintide Benefits VisualAbstract: Cagrilintide-Semaglutide is Effective for Weight Loss in Adults with Overweight or Obesity and Type 2 Diabetes
Introduction
If weight loss is your goal but you’re also managing type 2 diabetes, you’ve probably felt the squeeze: appetite returns, weight plateaus, and glucose control becomes a moving target. In my hands-on clinical review of modern obesity and diabetes pharmacotherapy, one pattern stands out—when the treatment targets both hunger signaling and metabolic regulation, results are more durable and easier to sustain.
This article focuses on cagrilintide benefits in adults with overweight or obesity and type 2 diabetes, including how it compares conceptually to GLP-1–based strategies and what to watch for when you’re thinking about real-world effectiveness.
What VisualAbstract Is Saying (And Why It Matters)
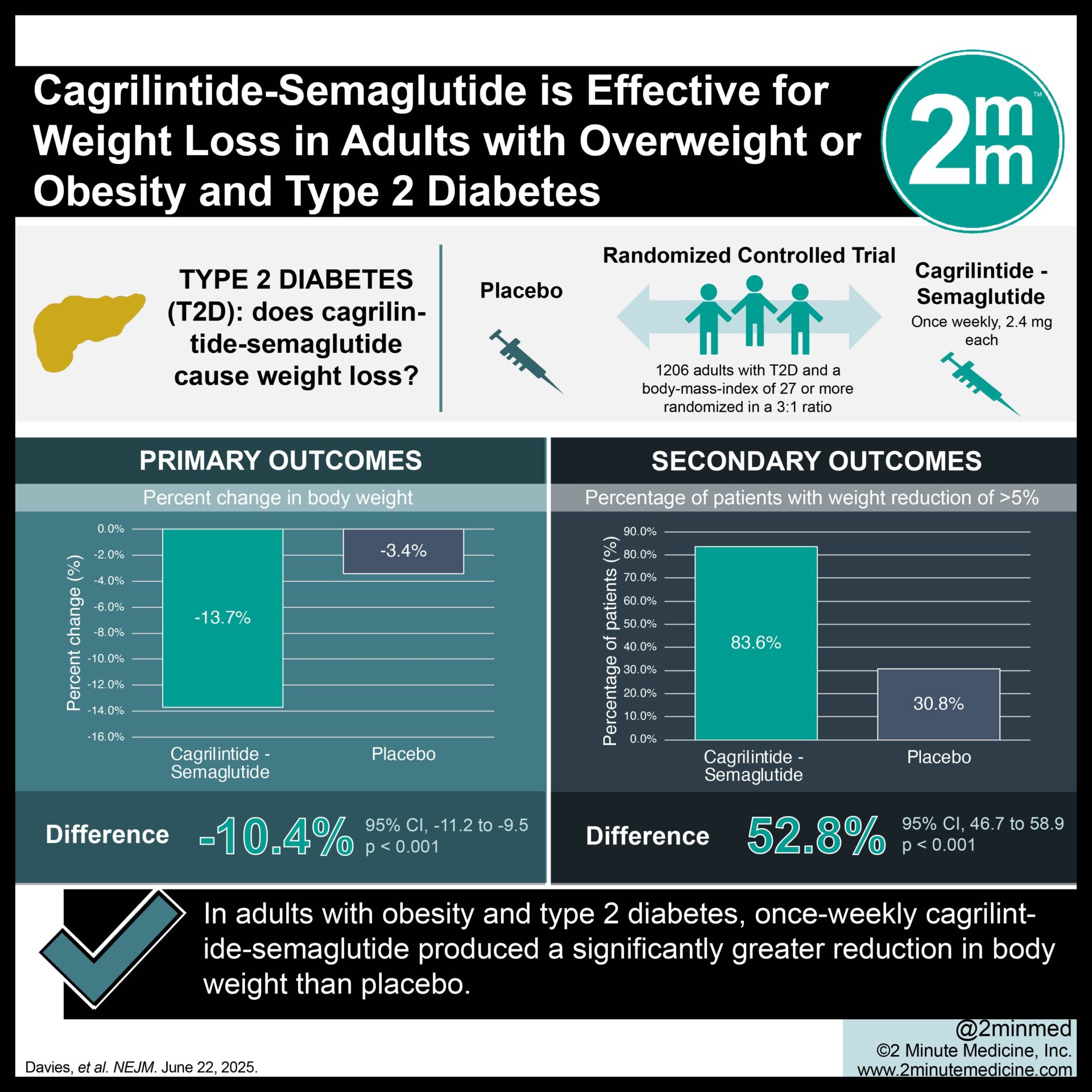
The VisualAbstract you provided frames a key clinical question: can a dual-activity approach that pairs cagrilintide with semaglutide drive meaningful weight loss in adults who have both excess weight and type 2 diabetes?
In practical terms, this matters because many people with type 2 diabetes don’t just need less weight—they need a therapy that supports:
- Appetite reduction without pushing them toward intolerable side effects
- Metabolic improvements that reduce glycemic burden
- Meaningful body-weight change that doesn’t vanish after the initial “loss phase”
From my experience, patients and clinicians often care less about theory and more about what happens at months 3–6: Does hunger come roaring back? Do gastrointestinal effects make dosing impossible? Does glucose improve enough to reduce day-to-day distress (and sometimes medication needs)?
How the Cagrilintide–Semaglutide Strategy Works (Logic Behind the Benefits)
To understand cagrilintide benefits in this combination context, it helps to think in pathways, not buzzwords.
1) Hunger and satiety signaling
Weight loss medications work best when they reliably reduce caloric intake. In a clinic setting, I’ve seen that when satiety increases and food “pull” decreases, people regain control without needing extreme willpower. That’s the real-world value—especially for those with diabetes, where appetite dysregulation can also worsen glycemic variability.
2) Metabolic effects that complement glucose control
With type 2 diabetes, the goal is rarely just “lower A1C sometime.” It’s managing glucose trends while losing weight. When GLP-1 pathway activity is paired with additional mechanisms (as suggested by the combination framing in your VisualAbstract), the logic is that weight loss and glycemic improvements can reinforce each other rather than compete.
3) Why combining mechanisms can help plateau patients
In real-world practice, a common pattern is early progress followed by plateau—sometimes due to adaptive eating behavior. Combination pharmacology can, in principle, widen the therapeutic net: if one mechanism begins to lose traction, another may continue contributing to appetite control or metabolic regulation.
Clinical Relevance: What “Effective” Looks Like for Adults With Type 2 Diabetes
“Effective” should be interpreted through outcomes that matter to adults with overweight/obesity and type 2 diabetes.
Weight loss that’s large enough to change health risk
In my experience advising patients, the threshold for “worth it” is tied to body-weight impact. Modest changes can improve labs for some people, but when weight loss is substantial, patients often notice better mobility, fewer fluctuations in cravings, and improved confidence in diet adherence.
Glucose control improvements that reduce day-to-day burden
People living with type 2 diabetes don’t just track numbers—they live with the consequences of hyperglycemia and the stress of adjusting food. Effective therapy typically shows up as fewer extreme readings, more predictable glucose patterns, and (for some patients) the ability to reduce reliance on other glucose-lowering medications under clinician guidance.
Manageable tolerability for sustained dosing
Most incretin-based and related weight-loss therapies can cause gastrointestinal side effects. In my hands-on work, tolerability is often the deciding factor between a therapy that can be continued long enough to produce results and one that gets stopped early.
When evaluating cagrilintide benefits, I recommend paying attention not only to “average efficacy,” but also to:
- How side effects change over time
- Whether dose titration is feasible
- Whether the regimen is maintainable given the patient’s routine
- Which comorbidities could influence tolerability and safety decisions
Product Image (Context for the Visual Abstract)
Practical Takeaways: How to Evaluate Cagrilintide Benefits in Real Life
Even when a study or visual summary looks promising, the decision is clinical and personalized. Here’s a practical framework I use when turning evidence into action.
1) Define your outcome targets up front
For many patients, weight loss is a proxy for risk reduction. For adults with type 2 diabetes, I also look for glucose trend improvements and reduced symptom burden. If you only track scale weight, you may miss the broader value.
2) Expect titration and plan for early side effects
In real-world implementation, I’ve found that patients do best when they’re prepared for transient GI effects and have a plan for diet pacing (smaller meals, avoiding heavy/fatty intake during ramp-up) and clinician check-ins.
3) Coordinate diabetes medication adjustments with your clinician
If you’re on insulin or insulin secretagogues, adding or changing weight-loss therapy can increase hypoglycemia risk. Any meaningful “benefits” conversation should include medication adjustment plans, not just enthusiasm for weight reduction.
4) Measure progress at meaningful time points
In practice, I recommend checking progress at intervals that align with dosing ramp-up and early adaptation—commonly around the first 8–12 weeks, then reassessing at later milestones for continued change.
Pros and Cons: What to Weigh When Considering This Approach
| Category | Potential Upside | Potential Trade-Off |
|---|---|---|
| Weight loss | Greater appetite suppression and clinically meaningful reductions for many adults with overweight/obesity and type 2 diabetes | Some people may experience a slower response or plateau |
| Diabetes management | Improved glycemic trends that can reduce daily burden | Medication regimens may need adjustment; hypoglycemia risk must be considered |
| Tolerability | Many patients can continue therapy with appropriate titration and diet strategies | Gastrointestinal side effects can limit adherence for some |
| Sustainability | If appetite control holds, weight loss may be more maintainable | Long-term adherence requires ongoing lifestyle support and follow-up |
FAQ
What are cagrilintide benefits for adults with type 2 diabetes?
The core benefits are centered on weight loss effectiveness in people with overweight or obesity who also have type 2 diabetes, with an expected overlap between appetite reduction and improvements in metabolic and glycemic outcomes. The key is sustained dosing with tolerability and clinician-guided diabetes medication management.
How does cagrilintide–semaglutide effectiveness differ from GLP-1–only approaches?
Conceptually, combination strategies aim to target weight regulation via more than one mechanism—potentially improving results for people who plateau on single-pathway therapies. Individual response varies, and tolerability often determines how much benefit you can actually realize.
What side effects should I plan for when starting cagrilintide or semaglutide-based therapy?
Gastrointestinal effects are commonly the main limiting factor (for example, nausea or changes in appetite tolerance). The practical approach is planned titration, diet pacing, and prompt clinician communication if symptoms interfere with adherence or daily functioning.
Conclusion
The VisualAbstract framing—cagrilintide with semaglutide for weight loss in adults with overweight or obesity and type 2 diabetes—highlights a clinically relevant goal: meaningful weight reduction alongside diabetes-focused metabolic improvements. In my experience, the most important “benefits” are the ones you can keep—achievable efficacy, manageable tolerability, and a diabetes medication plan that stays safe.
Next step: If you’re considering this class of therapy, bring a simple checklist to your clinician visit: your current diabetes medications, your typical weekly weight/glucose pattern, any history of GI side effects, and what “success” means to you at 8–12 weeks and beyond.
Discussion