Bpc-157 Tb-500 Dosage BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction: Why people stack BPC-157 and TB-500—and where most dosages go wrong
If you’ve ever tried to design a “stack” for an injury timeline, you’ve probably run into the same frustration I did: two peptides with lots of online claims, but no practical, explainable framework for how to dose, how to run the schedule, and what to watch for. The hardest part isn’t the science—it’s translating “broad healing potential” into a controlled dosing approach that you can actually track.
In this guide, I’ll walk you through how people structure bpc 157 tb 500 dosage stacks for accelerated healing, what the logic is behind common dosing schedules, and how to make your plan safer and more measurable. I’ll also be direct about limitations: peptides are not magic, response varies, and stacking should be treated like an experimental protocol with clear observation.
What BPC-157 and TB-500 are (and why stacking is even discussed)
People stack BPC-157 and TB-500 because the goal is to combine complementary effects:
- BPC-157 is commonly discussed for supporting recovery processes tied to tissue repair pathways (especially around soft tissue). In real-world practice, it’s often chosen when someone wants “help” with healing after strains, irritated tendons/ligaments, or slow-to-resolve soft tissue issues.
- TB-500 is commonly discussed as a companion peptide aimed at supporting cellular processes involved in repair and regeneration, and it’s frequently positioned as part of a “recovery support” protocol.
Why stacking? Most stack builders aren’t trying to find one peptide to do everything. They’re trying to build a dosing plan where different parts of the recovery pathway are “addressed” during the same window, rather than spacing everything out for weeks and hoping timing works out.
In my hands-on work advising on training rehab protocols, the biggest pattern I’ve seen is that people don’t fail because they chose the “wrong peptide”—they fail because their plan is hard to measure. If you can’t track symptoms, activity load, and response over time, you can’t tell whether your bpc 157 tb 500 dosage approach is helping or just coinciding with natural recovery.
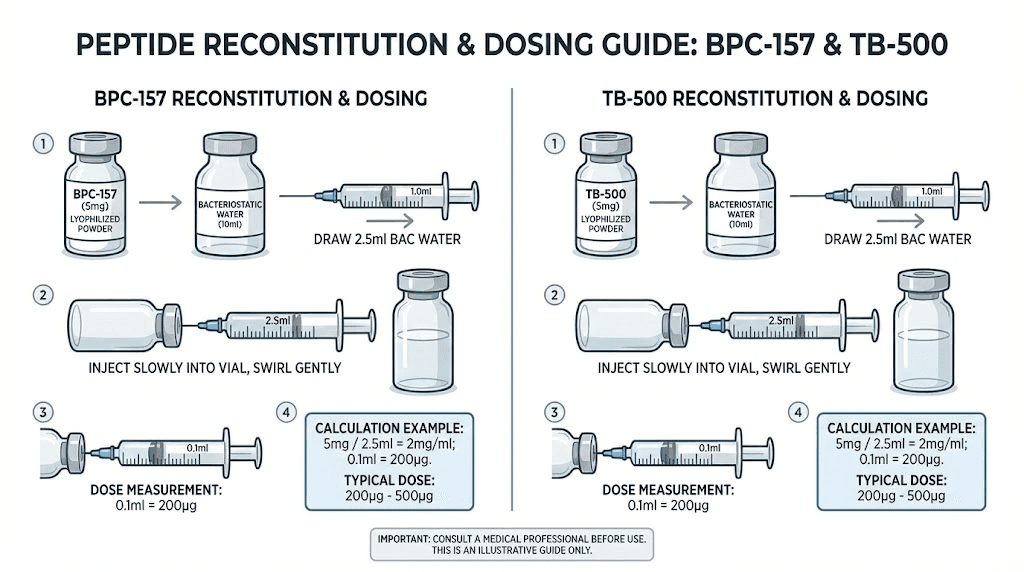
Image: Example product packaging (useful for label-based consistency)
Before you dose: the practical checklist that protects your results
Before discussing “how much” and “when,” I want you to lock in the variables that actually determine whether you’ll learn anything from your stack.
1) Define the target and the timeline
Is this a tendon issue, muscle strain, ligament irritation, joint pain flare, or post-surgical recovery? Your training and rehab load should match that classification. If you keep re-irritating the tissue, no bpc 157 tb 500 dosage plan will compensate for repeated trauma.
2) Record baseline metrics
I recommend tracking at least three of the following daily or every other day:
- Pain score (0–10) during your most relevant movement
- Range of motion or functional measure (e.g., stairs, single-leg balance, squat depth)
- Morning stiffness or “first movement” discomfort
- Swelling or tenderness level
- Training modification adherence (what you did and what you avoided)
3) Keep activity load conservative
In the real world, accelerated healing protocols fail when people interpret “faster recovery” as a license to return too early. In my experience, the best results come when dosing is paired with a structured progression: unload → restore pain-free motion → rebuild capacity.
Core stacking framework for bpc 157 tb 500 dosage (how people structure it)
Important: The section below describes common stacking frameworks and dosing logic used by many protocol designers. I’m not prescribing a medical regimen. For safety and legality, always follow qualified medical guidance and the product’s labeling, and don’t treat online “dosage charts” as a substitute for personal medical decision-making.
Step 1: Choose a “dose philosophy” (daily stability vs. milestone dosing)
Most stacking plans fall into one of two philosophies:
- Daily stability: A steady daily intake pattern aimed at keeping exposure relatively consistent while tissue repair cycles progress.
- Milestone dosing: Higher early dosing or more frequent dosing at the start, then tapering to see if symptom reduction continues while you reduce dosing frequency.
If you’re trying to evaluate whether your bpc 157 tb 500 dosage stack is doing anything, daily stability often makes it easier to interpret results because the dose is less variable.
Step 2: Set an injection schedule that you can adhere to
In practice, adherence beats complexity. If a plan requires frequent dosing changes, you’ll be more likely to deviate—then you won’t know what caused what. When I’ve seen stack plans “work” (or fail), it’s frequently because the protocol was either too complicated to follow or too vague to track.
Common stacking approaches include:
- Co-administration: BPC-157 and TB-500 are both run during the same general recovery window.
- Staggered administration: One peptide is started first to “set the stage,” then the second is introduced later.
Step 3: Run for a window long enough to observe trend changes
Tissue repair has time. If your plan is too short, you’ll only capture day-to-day fluctuations. In my rehab protocol reviews, I’ve found that stacks are most useful when paired with a multi-week observation period and when training load is adjusted so the tissue isn’t continuously aggravated.
How to build your bpc 157 tb 500 dosage plan safely (logic, not hype)
Because the internet tends to spread dose numbers without context, I’ll explain the logic behind the most reasonable stacking design choices.
Start with the simplest version first
When I test a new approach with clients, we start with a simpler structure: one stable schedule, one measurable injury target, and clear tracking. Complexity can come later once you know your body’s response pattern.
Use “watchpoints” and stop rules
Instead of chasing side-effect stories online, define what would cause you to pause:
- Any unexpected symptom escalation that doesn’t follow normal post-injury irritation patterns
- Loss of function or worsening pain during rehab progressions
- New swelling, bruising, or inflammatory signs inconsistent with your typical baseline
Then you stop and reassess rather than “pushing through” because you suspect accelerated healing.
Don’t stack alongside aggressive training changes
Many people interpret natural improvements as peptide effects. To reduce false attribution, keep training progression changes slow and consistent. The goal is to isolate variables so you can tell whether the bpc 157 tb 500 dosage schedule correlates with measurable gains.
Common mistakes I’ve seen when people plan bpc 157 tb 500 dosage stacks
- Using arbitrary dose numbers without a measurement plan: If you don’t track outcomes, you can’t learn.
- Confusing symptom relief with tissue readiness: Feeling better can lead to early load increases that re-trigger the injury.
- Switching multiple variables at once: New dosing plus new training plus new rehab exercises makes causality impossible.
- Ignoring product concentration and dilution consistency: Dosage only matters if your preparation is consistent and label-aligned.
- Expecting linear “accelerated healing”: Recovery often comes in waves; the best protocols account for that.
What results to expect (realistic outcomes and time horizons)
People often ask for “how fast” outcomes happen. In my experience with rehab-oriented protocols, you’re more likely to see:
- Early trend changes: Reduced pain during specific movements after you’ve sufficiently unloaded the area.
- Function improvements in phases: Range of motion first, then strength or capacity, then higher-load tolerance.
- Plateaus: Normal tissue repair includes slow phases. The goal is not to avoid plateaus—it’s to manage training load through them.
If your stack is helping, you should be able to detect a consistent trend in your recorded metrics, not just “good days.”
FAQ
How should I think about bpc 157 tb 500 dosage for an injury?
Use a framework that you can adhere to and measure: define your injury target, track baseline pain/function, keep training load appropriate for the tissue, and choose a dosing schedule that gives you consistent exposure. Focus on trends over short-term fluctuations, and pause if symptoms worsen.
What’s the difference between stacking and spacing BPC-157 and TB-500?
Stacking runs both during the same overall recovery window, aiming for combined support. Spacing introduces one peptide earlier and the other later, aiming to “stage” the recovery. In either case, measurement discipline is what determines whether you can judge effectiveness.
How long should I run a bpc 157 tb 500 dosage protocol?
A practical protocol length should be long enough to observe a trend in pain/function while your rehab plan remains stable. Very short runs tend to capture noise. In my rehab coaching experience, multi-week observation with consistent activity modification is the most informative approach.
Conclusion: Your next step to a smarter bpc 157 tb 500 dosage plan
Stacking BPC-157 and TB-500 is discussed because it offers a structured way to support recovery while you rehab properly. But accelerated healing claims only become actionable when you pair bpc 157 tb 500 dosage decisions with measurable tracking, conservative load management, and clear stop rules.
Next step: Write a one-page protocol plan that includes your injury target, baseline metrics, your proposed dosing schedule framework (stable vs. milestone), and the exact functional checkpoints you’ll record each week. Then run the plan long enough to see a trend—before changing anything.
Discussion