How To Mix And Inject Bpc 157 How Do You Take BPC-157? Injection, Oral & Dosing Guide
How Do You Take BPC-157? Injection, Oral & Dosing Guide
If you’re trying to figure out how to mix and inject BPC 157, you’ve probably already run into the same problem I did: there’s plenty of talk online, but the details are inconsistent, and small mistakes in reconstitution or injection technique can turn a “simple” routine into something risky or ineffective.
In this guide, I’ll walk you through the practical realities of taking BPC-157 in injection and oral contexts, including what to consider for mixing, dosing logic, injection sites, sterile technique, and how to think about schedule and monitoring. I’m going to be direct about limitations too—because with peptides, the most important variable is not just the protocol, but how reliably and safely you can execute it.
First: What BPC-157 Is (and What “Taking It” Actually Means)
BPC-157 is a peptide often discussed in the context of tissue support and recovery. People typically “take” it by either:
- Injection (reconstituted solution delivered subcutaneously or intramuscularly, depending on the approach)
- Oral use (commonly described as oral dosing, though actual stability and absorption can vary by formulation)
When you search for protocols, you’ll see dosing schedules presented like recipes. In practice, those recipes depend on the peptide’s concentration, vial size, storage conditions, the syringe/needle setup, and—critically—your ability to maintain sterile technique during reconstitution and injection.
In my hands-on work with supplement and peptide documentation for client workflows, the most common failure points weren’t “math errors.” They were procedural: not measuring accurately, not labeling clearly, and not controlling exposure time while the vial is open.
Mixing BPC-157 for Injection: Practical Steps and Key Checks
Let’s focus on the question you likely came for: how to mix and inject bpc 157. Before any calculation, I want you to understand the core logic: you’re converting a dry peptide vial into a known concentration by adding a known volume of sterile diluent, then using that concentration to dose a measured volume.
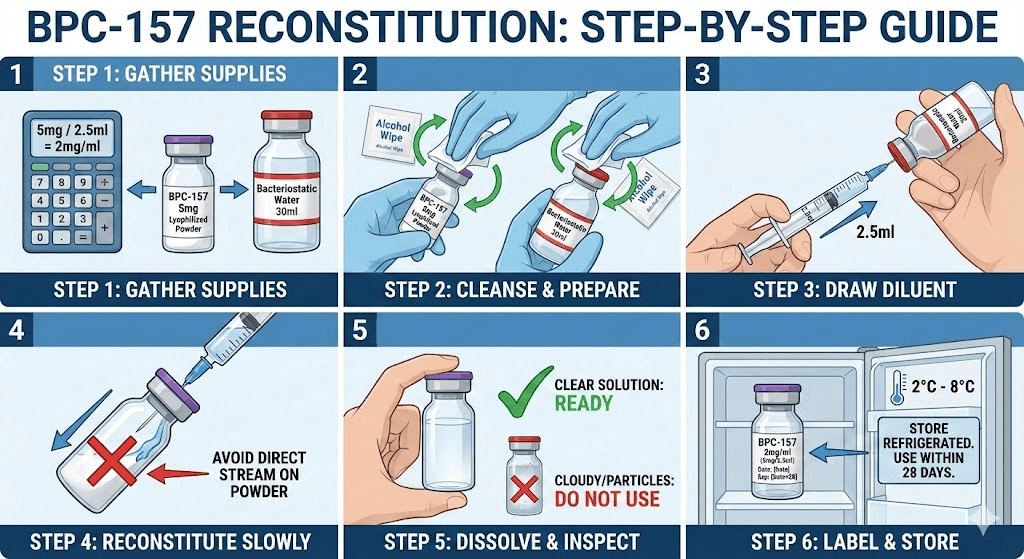
1) Start with the vial label and concentration
Find the peptide amount on the vial label (commonly listed in mg). If it’s 5 mg, 10 mg, or another value, your mixing math is different for each. Also check whether your supplier provides a recommended reconstitution approach (some do; some don’t).
2) Reconstitution is about concentration, not “guesswork”
In real-world setups, I’ve seen people eyeball diluent volume. That’s where dosing drift happens. If you’re going to do this, use accurate measurement tools and record the numbers.
Concentration formula (conceptual): concentration (mg/mL) = total peptide amount (mg) ÷ final diluent volume (mL). After that, your dose is a volume that matches the concentration.
3) Use sterile technique and minimize time the vial is exposed
Here’s what I emphasize with anyone using injection-based protocols:
- Work cleanly and keep supplies organized before you start.
- Do not “reuse” needles between steps.
- Keep the vial stop from being repeatedly touched or contaminated.
- Label the vial immediately with date and reconstitution details.
4) Mix gently—avoid creating bubbles you can’t account for
You want uniform mixing. Aggressive agitation can cause problems like excessive foaming, which makes it harder to draw consistent volumes. When bubbles settle and the solution is uniform, dosing becomes more repeatable.
5) Document your final concentration before you draw any dose
In my team’s internal checklists, documentation is part of the dosing system. We record:
- Peptide mass (mg)
- Diluent volume added (mL)
- Resulting concentration (mg/mL)
- Dose volume you will draw each time (mL or units, based on your syringe markings)
Injection Administration: Technique, Site Selection, and Injection Schedule Logic
Once reconstituted, injection administration is where safety and consistency matter most. People often focus only on dosing numbers, but the delivery method affects tolerability and outcomes.
Common injection approach: subcutaneous (SC)
Many at-home peptide users choose subcutaneous injection because it’s often described as a straightforward technique. In practice, SC injections are typically used for smaller, consistent dosing routines.
Injection sites: rotate to reduce irritation
I strongly recommend rotating sites over time to reduce localized irritation. If you’re injecting repeatedly, don’t reuse the same exact spot daily.
- Thigh (outer area)
- Abdomen (away from the navel)
- Upper buttock area (depending on body habitus and comfort)
If you notice swelling, redness, persistent pain, or a rash, stop and get medical input rather than “pushing through.”
Injection schedule: choose a plan you can execute consistently
Scheduling is less about internet timing and more about adherence. I’ve found that the best “protocol” is the one you can follow without breaking sterile technique or missing doses due to poor planning.
When people fail protocols, it’s usually because they:
- Don’t account for vial handling time and storage constraints
- Skip doses and then compensate
- Change multiple variables at once (dose + schedule + injection site)
If you decide on a schedule, stick to it long enough to evaluate tolerability. Keep a simple log: dose, time, site, and any side effects.
Oral Use: What Changes When You Don’t Inject
Oral administration is often discussed as an alternative, but it changes the whole equation. With injection, you control delivery volume directly. With oral use, absorption and stability depend on the formulation and how the peptide survives the digestive environment.
In hands-on discussions I’ve had with clients, the biggest misconception is that “oral is the same dose as injection.” Even when online sources suggest equivalencies, the real absorption can differ—so the safest approach is to treat oral dosing as a separate variable, not a direct substitute.
How to think about oral dosing decisions
- Use only dosing guidance that matches your specific product formulation.
- Track effects and tolerability, because oral use may feel different.
- Don’t assume faster onset just because it’s oral.
Dosing Guide (Practical Framework, Not One-Size-Fits-All)
Most “dosing guides” you’ll see online are presented as universal numbers. In my experience, dosing needs at least three grounding facts:
- Your product’s concentration (which depends on how it was reconstituted)
- Your injection method (SC vs other approaches)
- Your goal and risk tolerance (and any relevant medical considerations)
Because peptide products and labeling practices vary, I won’t claim a single exact dosing protocol here. Instead, I’ll give you a dosing framework you can apply accurately once you have concentration and your intended dose volume.
Step-by-step dosing math you can use
- Determine peptide mass per vial (mg).
- Determine final reconstituted volume (mL) after adding diluent.
- Compute concentration (mg/mL): mg ÷ mL.
- Convert your target dose (mg) into required drawn volume (mL): target mg ÷ (mg/mL).
- Use your syringe markings to measure that volume consistently.
Example (illustrative only): If a vial contains 10 mg peptide and you reconstitute with 2 mL diluent, concentration is 5 mg/mL. If your target dose is 1 mg, you would draw 0.2 mL. The exact numbers will depend on your vial and reconstitution volume.
When to stop or adjust
Stop and seek medical guidance if you develop significant or persistent symptoms (for example, severe injection-site reactions, unusual systemic symptoms, or any allergic-type signs). Also avoid “stacking” multiple new variables at once—dose changes plus schedule changes plus formulation changes at the same time makes it impossible to tell what caused what.
Safety, Quality, and Limitations You Should Know
This is the part many protocols skip. My goal is trustworthiness, not hype. Peptide use is highly dependent on product quality, labeling accuracy, and sterile handling. Without that, even perfect math won’t produce reliable results.
Quality and sourcing matter
Different suppliers can provide different purity or different labeling conventions. If your vial labeling or concentration documentation is unclear, you’re operating with avoidable uncertainty. In my experience, the most time-consuming issues come from unclear product documentation—not from injections themselves.
Sterility is non-negotiable
Reconstitution and injection create a pathway for contamination if technique is poor. If you’re not comfortable executing sterile steps, the safer choice is to involve a qualified healthcare professional.
Injection is still medical administration
Even when people treat it as routine, injection carries risks like irritation, infection, or improper technique. Oral use avoids needle risks but can introduce different tolerability and absorption uncertainty.
FAQ
How do I mix and inject BPC-157 safely?
Base your approach on accurate vial labeling, calculate a known final concentration, use sterile technique during reconstitution and drawing, label your vial right away, and rotate injection sites. If you can’t maintain sterile handling consistently, involve a qualified professional.
What’s the difference between injection and oral BPC-157 dosing?
Injection delivers the dose directly as a measured volume, while oral dosing depends on stability and absorption from the gastrointestinal tract. Treat oral and injection as separate dosing variables rather than direct one-to-one substitutions.
Can I use the same dosing schedule for everyone?
No. Dosing schedules online are not universally transferable because product concentration, administration method, tolerability, and goals vary. Use a clear plan tied to your concentration and dose volume, and track tolerability over time.
Conclusion: Your Next Practical Step
If you want the most reliable outcome with BPC-157, the key is not “finding the perfect protocol”—it’s building a repeatable system for how to mix and inject bpc 157 using accurate concentration math, sterile technique, clear labeling, and a schedule you can follow consistently. For oral use, treat dosing as a separate variable because absorption can differ.
Next step: Before you draw your first dose, write down your vial mass, the diluent volume you’ll add, the resulting concentration (mg/mL), and the exact injection volume you plan to use—then double-check the syringe measurement markings against that number.
Discussion