Can b12 injections increase ferritin levels Pernicious Anemia: Definition, Symptoms, Causes & Treatment
Introduction
If you’ve ever had iron labs come back “off” and then wondered whether B12 therapy could be involved, you’re not alone. In clinic, I frequently see patients who start treatment for pernicious anemia and later notice changes in other labs—sometimes including ferritin. That’s why people ask a precise question: can b12 injections increase ferritin levels? In this guide, I’ll explain what pernicious anemia is, why ferritin may shift during treatment, what to watch for on labs, and how clinicians typically approach diagnosis and treatment.
Pernicious Anemia: Definition and What Makes It Different
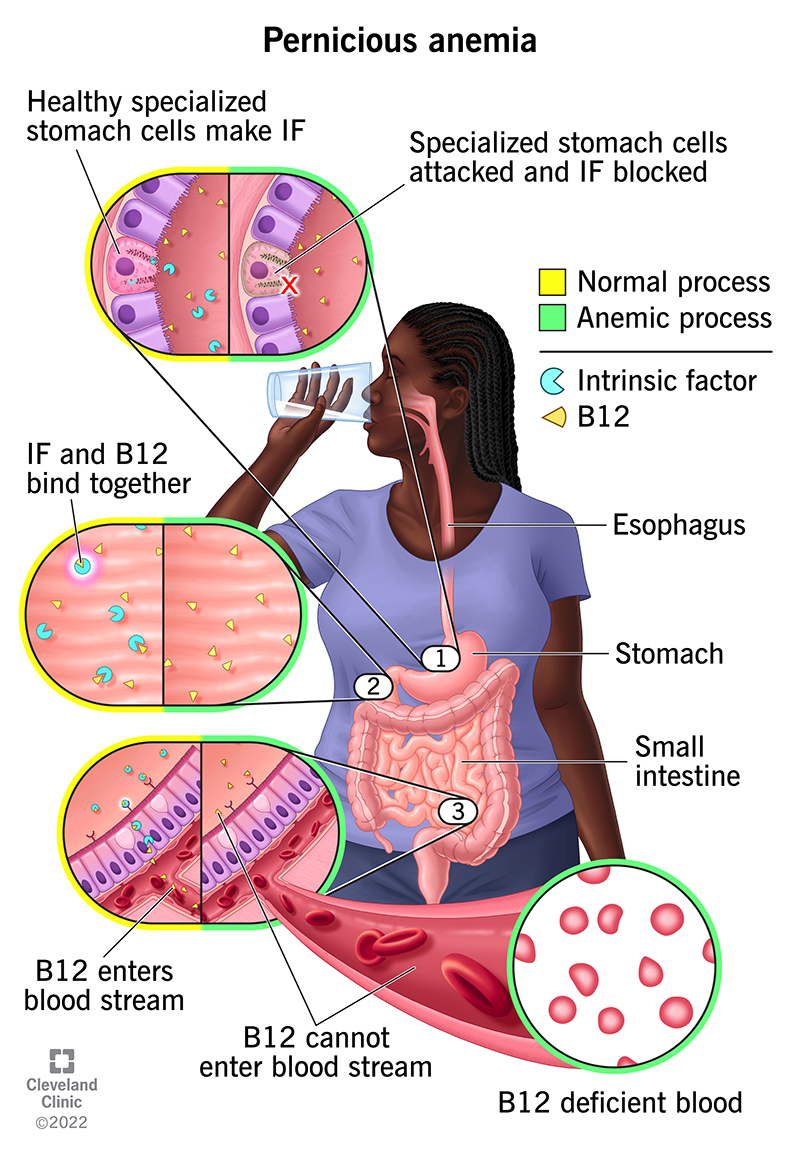
Pernicious anemia is a type of megaloblastic anemia caused by impaired absorption of vitamin B12. The most common mechanism is autoimmune destruction of gastric cells (and related intrinsic factor), which is needed for B12 absorption in the small intestine.
In my hands-on experience, the “aha” moment for many patients comes when they realize pernicious anemia isn’t just “low B12.” It’s a specific absorption problem with a predictable treatment path. That’s important because the response to therapy (including lab trends) differs from other causes of anemia.
How B12 deficiency leads to anemia
When B12 is insufficient, DNA synthesis in red blood cell precursors becomes inefficient. This produces fewer, larger red blood cells (megaloblastosis), which is why pernicious anemia is commonly linked to elevated MCV and characteristic blood count patterns.
Symptoms of Pernicious Anemia: What to Look For
Pernicious anemia can develop gradually, and symptoms often reflect both anemia and (in some cases) neurologic effects from prolonged B12 deficiency. Common symptoms include:
- Fatigue and low energy
- Shortness of breath with exertion
- Dizziness
- Pale skin
- Glossitis (sore, smooth tongue)
- Tingling or numbness in hands/feet (neurologic symptoms)
- Balance issues
- Memory or concentration difficulties
One practical lesson I’ve learned: neurologic symptoms can lag behind lab changes. So even when blood counts start improving, clinicians still take symptom persistence seriously.
Causes and Risk Factors
Most cases relate to autoimmune mechanisms that reduce intrinsic factor or damage the stomach lining. Other associated factors and risks include:
- Autoimmune conditions (e.g., autoimmune thyroid disease, type 1 diabetes in some patients)
- Gastritis (including autoimmune gastritis)
- Family history of autoimmune disease (variable)
- Age (risk increases with older age)
How Treatment Works: B12 Injections and Expected Lab Changes
Why injections are commonly used
Because pernicious anemia involves impaired absorption, clinicians often use B12 injections (or sometimes high-dose oral B12 in select cases) to bypass the need for intrinsic factor–mediated uptake.
In real-world practice, the treatment goal is twofold: correct anemia and prevent or halt neurologic decline. Monitoring focuses on blood counts and B12 status, and clinicians also reassess other nutrient deficiencies that may coexist.
What improving B12 actually changes
When B12 levels normalize, the bone marrow can resume proper DNA synthesis. Over time, red blood cell indices and hemoglobin typically improve. However, iron stores—often assessed through ferritin—don’t always move in a straightforward way, because ferritin reflects multiple processes.
The Core Question: Can B12 Injections Increase Ferritin Levels?
Short answer: they can indirectly contribute to ferritin changes, but B12 injections are not a direct “iron booster,” and ferritin may rise, fall, or remain the same depending on what’s causing the low ferritin (if it is low).
Why ferritin isn’t determined by B12 alone
Ferritin is an iron-storage protein, and its blood level is influenced by:
- Iron intake and absorption (and whether you have true iron deficiency)
- Ongoing blood loss (common in some adults)
- Inflammation or infection (ferritin often rises as an “acute-phase reactant,” even when iron is low)
- Erythropoiesis (red blood cell production) demand for iron
In my experience reviewing lab patterns, it’s common for patients to have more than one issue at once—such as B12 deficiency plus iron deficiency from dietary factors, malabsorption, or chronic blood loss.
Mechanisms where B12 therapy can indirectly raise ferritin
Here are realistic pathways by which B12 injections may coincide with higher ferritin:
- Improved red blood cell production stabilizes iron handling: As marrow activity normalizes, the body’s utilization patterns can shift. If iron intake is adequate (or iron deficiency is resolving), ferritin may recover.
- Correcting mixed deficiencies: Some patients with pernicious anemia also have iron deficiency. If they start iron supplementation (or dietary iron improves) at the same time as B12, ferritin can rise during follow-up. People often attribute the change to B12 alone, even though the iron plan matters most.
- Resolution of nutritional stress: When overall nutrition and hematologic function improve, iron stores may gradually rebuild—again, typically with adequate iron availability.
Why ferritin might not rise (or could look “worse” temporarily)
Conversely, ferritin may not increase even with successful B12 injections:
- Unaddressed iron deficiency: If iron stores are depleted and not being replenished, ferritin can remain low.
- Ongoing inflammation: Ferritin can behave differently in inflammatory states, sometimes masking iron deficiency.
- Concurrent blood loss: Without stopping the underlying loss, iron stores may not rebuild.
- Timing differences: Ferritin changes may lag behind improvements in B12-related anemia markers.
What clinicians typically monitor alongside B12
To interpret ferritin properly in a patient with pernicious anemia, I look for a broader iron panel and relevant context, such as:
- Ferritin
- Serum iron
- Total iron-binding capacity (TIBC) and/or transferrin saturation
- Complete blood count (CBC) including hemoglobin and MCV
- Vitamin B12 level and, in some settings, supportive markers
This is the practical point: ferritin interpretation is strongest when it’s part of a pattern, not a single number.
Causes of Low Ferritin in People With Pernicious Anemia
If your ferritin is low, it’s worth considering why. In real practice, low ferritin with pernicious anemia can reflect:
- True iron deficiency from inadequate intake
- Reduced absorption related to gastrointestinal conditions
- Chronic blood loss (which must be evaluated based on age and risk)
- Mixed anemia (B12 deficiency plus iron deficiency at the same time)
The key lesson: even if B12 injections correct anemia, ferritin won’t normalize if iron deficiency is still present and not treated.
Treatment Strategy: What “Good Care” Looks Like
Management usually involves three parallel tracks: treat B12 deficiency, assess anemia response, and evaluate iron status (and any contributing causes).
B12 treatment (typical clinical approach)
- Start B12 injections to bypass absorption problems.
- Plan follow-up labs to confirm hematologic response and B12 repletion.
- Address neurologic symptoms promptly (especially if present).
Iron evaluation and supplementation (when appropriate)
- If ferritin and transferrin saturation indicate iron deficiency, clinicians often recommend iron supplementation or dietary changes.
- If inflammation is suspected, interpretation may require additional context beyond ferritin alone.
Identify underlying contributors
When ferritin is low, good care includes looking for reasons iron stores are depleted (dietary issues, absorption problems, or blood loss). The correct workup depends on your age, sex, symptoms, and medical history.
FAQ
1) How long after B12 injections would ferritin increase?
Ferritin changes can lag because ferritin reflects iron storage, not just B12 repletion. If ferritin is low due to iron deficiency and iron intake/supplementation is adequate, you might see improvement over weeks to a few months. If ferritin doesn’t rise, it usually means iron deficiency persists or the ferritin signal is being influenced by inflammation or ongoing loss.
2) Can B12 injections raise ferritin if I’m not iron deficient?
Typically, ferritin isn’t expected to rise meaningfully just from B12 repletion alone. If your iron stores are already adequate, B12 injections primarily correct the megaloblastic anemia pathway; ferritin may remain stable unless there are other concurrent factors.
3) What labs best clarify whether my low ferritin is from iron deficiency?
Ask your clinician about pairing ferritin with serum iron, TIBC (or transferrin), and transferrin saturation, plus a CBC trend. This combined picture helps distinguish iron deficiency from inflammatory patterns and helps identify mixed anemia.
Conclusion
Pernicious anemia is a B12 absorption disorder, and B12 injections reliably correct the megaloblastic anemia component. But can b12 injections increase ferritin levels? The most accurate way to think about it is indirect: ferritin may rise if iron deficiency is also present and being replenished, but B12 injections aren’t a substitute for addressing the underlying iron problem.
Next step: If your ferritin is low, request a coordinated review of your iron panel (ferritin, serum iron, TIBC, transferrin saturation) alongside B12 and CBC trends, so treatment targets the actual driver—whether it’s mixed deficiencies, inflammation, or blood loss.
Discussion