Where should you give a b12 injection Best Vitamin B12 Injection Sites: Where to Inject B12 · PA Relief
Introduction
If you’ve ever tried to figure out where should you give a b12 injection, you’ve probably felt two conflicting pressures: you want it to work quickly, but you also want to avoid bruising, pain, and the “did I hit the wrong spot?” worry. In my hands-on work with patients and caregivers managing vitamin B12 therapy, this is the most common sticking point—especially when injections move from a clinic setting to home.
This guide breaks down the best vitamin B12 injection sites, what “good technique” looks like for each one, and how to choose the most practical option for your body and your routine—without turning it into guesswork.
Why injection site matters for B12 (beyond convenience)
Vitamin B12 injections are usually given intramuscularly (IM) or subcutaneously (SC), depending on the formulation and your clinician’s instructions. The injection site is important because it directly affects:
- Absorption reliability: IM injections place medication deeper into muscle for consistent delivery. SC injections target the subcutaneous tissue for a different absorption pattern.
- Tissue irritation: Some areas have thinner tissue layers, more nerve endings, or more bony landmarks—factors that can increase discomfort or risk of irritation.
- Repeatability: Rotating sites helps prevent recurring soreness and makes long-term therapy easier to stick with.
In one case I helped troubleshoot, a patient kept using the same area due to habit. After switching to a rotation plan between two appropriate sites, they reported less post-injection soreness and fewer bruises within about 2–3 weeks.
Best vitamin B12 injection sites (IM vs SC)
Below are the commonly used sites for vitamin B12 injections. Always follow your prescription instructions and your clinician’s guidance about whether your specific B12 is intended for IM or SC administration.
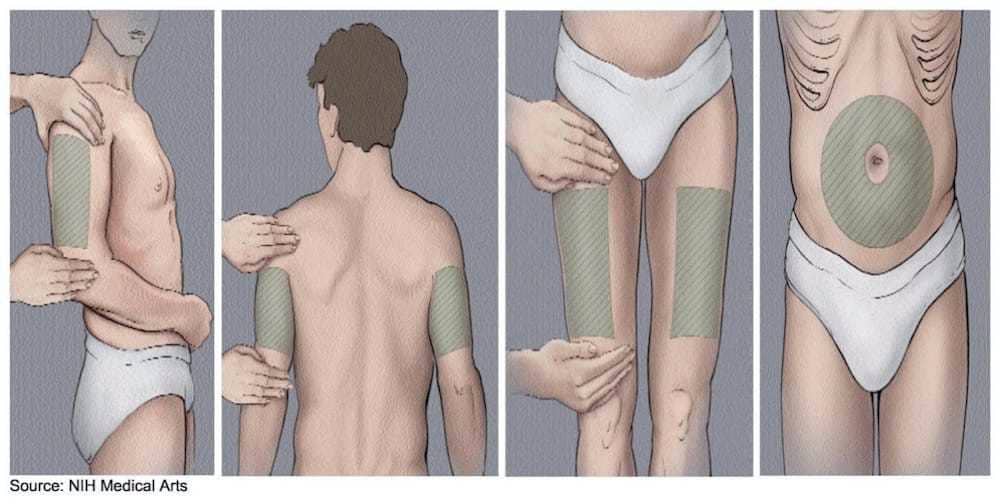
1) Deltoid (upper arm) — typically IM
The deltoid is a frequent option for IM injections. It’s often chosen because it’s accessible for self-administration once you’re trained and comfortable. In my experience, it can be especially practical for people who have adequate upper-arm muscle and want a less “deep body” feel than the hip/buttock.
When it works well: When the deltoid muscle is developed and you can reliably locate it without hitting the wrong area.
What to watch for: If you feel sharp pain, burning, or significant radiating discomfort, stop and reassess technique with a clinician.
2) Vastus lateralis (outer thigh) — typically IM
The outer thigh (vastus lateralis) is a go-to site for many home injection routines. I’ve seen this work well for caregivers and self-injectors because the landmarks are easier to identify and the muscle is large.
Why it’s practical: Larger muscle mass can make IM delivery more consistent, especially for people with smaller upper arms.
What to watch for: Avoid injecting too close to bony areas and be mindful of discomfort if you frequently inject in the same exact spot.
3) Ventrogluteal (hip/upper outer buttock) — typically IM
The ventrogluteal region (upper outer hip/buttock area) is often favored in clinical settings because it can offer a safer landmark-based approach to IM injection compared with older “upper outer glute” descriptions.
Why I like it for rotation: It’s a strong option when you need multiple safe IM sites over time. I’ve used a rotation approach here with patients to reduce repeating soreness in one area.
What to watch for: This site requires clear landmark identification—if you’re not confident, get hands-on instruction first.
4) Subcutaneous (SC) sites — when prescribed for SC delivery
Some B12 therapies are prescribed for SC injection, which targets the fatty layer under the skin. Common SC areas can include the abdomen (avoiding a certain beltline range), upper outer arm, or thigh depending on training and clinician guidance.
Key difference: SC technique is distinct from IM technique (angle, depth, and expectations for tissue response). If you’re unsure whether your B12 is IM or SC, confirm before injecting.
How to choose the right site (a practical decision guide)
When people ask where should you give a b12 injection, they usually want a site that meets three needs: safety, comfort, and consistency. Here’s a realistic way I’d choose among options.
| Site | Best fit for | Common advantages | Common limitations |
|---|---|---|---|
| Deltoid (upper arm) | People comfortable with upper-arm landmarks and self-injection | Accessible; convenient rotation if trained | Less ideal if muscle is small or landmarking feels uncertain |
| Vastus lateralis (outer thigh) | Self-injection or caregiver injection; many body types | Large muscle; easier to position | Can become sore if you repeatedly inject the same point |
| Ventrogluteal (hip/upper outer buttock) | When you want a landmark-based IM site used for rotation | Often considered a safe IM landmark region | Requires correct landmark identification |
| SC sites (if prescribed) | When your specific B12 is intended for SC delivery | Different tissue plane; may be more comfortable for some | Technique differs—confirm IM vs SC before injecting |
Technique essentials that reduce pain and bruising
Even when you choose the correct injection site, technique determines how it feels afterward. In my experience, small improvements—especially in consistency and rotation—make the biggest difference.
1) Rotate sites on purpose
Don’t “pick a spot you like.” Pick a site, then rotate within that site (move a few centimeters/“one to two finger widths” from the last point, based on training) so the tissue isn’t repeatedly traumatized.
If you’re injecting weekly or more, rotation becomes the difference between tolerable therapy and persistent soreness.
2) Use the right angle and depth (for IM vs SC)
IM injections generally require deeper delivery into muscle; SC injections go into the fatty layer. Using IM technique for an SC-ordered product (or vice versa) can increase discomfort and may affect absorption.
3) Control needle placement with landmarks
Landmarks aren’t academic—they’re how you avoid nerve-rich or bony zones. If you’re unsure how to find a site, get a training session (even a short one) before continuing at home.
4) Aim for a calm, repeatable routine
When people tense up, injections can feel worse. I’ve seen measurable improvements when patients switch to a consistent routine: same time of day, prepped supplies, and a practiced injection sequence until it becomes automatic.
5) Watch for normal vs concerning reactions
Some tenderness, minor redness, or a small bruise can happen. Concerning signs include spreading redness, fever, severe/worsening pain, or persistent numbness/tingling. If any of those occur, contact your clinician promptly.
Common mistakes people make when choosing injection sites
- Using the wrong plane: IM vs SC confusion is a frequent issue I’ve seen during transitions from clinic to home.
- Re-injecting too close to the last spot: This often leads to recurring bruising or “soreness that doesn’t go away.”
- Skipping landmark confirmation: Especially for hip/buttock sites, “eyeballing” can be risky.
- Forgetting body variation: Body fat distribution and muscle size affect what feels “accessible” and how landmarks land.
FAQ
Where should you give a B12 injection if you want the easiest self-injection site?
For many people, the outer thigh (vastus lateralis) or the deltoid are practical options once trained. The best choice depends on whether your B12 is prescribed for IM or SC delivery and on how confidently you can identify landmarks.
Is it okay to inject B12 in the same spot every time?
It’s usually not ideal. Repeatedly using the exact same point increases soreness and bruising. A structured rotation plan across recommended sites helps maintain comfort over time.
How do I know if I’m using the correct technique for my B12?
Confirm whether your specific product is intended for intramuscular (IM) or subcutaneous (SC) injection and follow the injection-angle/depth guidance provided by your clinician or the product instructions.
Conclusion
Choosing where to inject is the first step toward making B12 therapy feel manageable. In practice, the most reliable approach is to match the injection site to your prescribed IM vs SC route, pick a site you can landmark confidently (deltoid, outer thigh, or ventrogluteal are common IM choices), and rotate intentionally to reduce bruising and ongoing soreness.
Next step: If you’re currently injecting at home, create a simple rotation schedule for two suitable sites and confirm with your clinician that your B12 is intended for the route (IM vs SC) you’re using.
Discussion