Bpc 157 Tb 500 Capsules Vs Injection BPC-157 vs TB-500: Complete Comparison (2026)
If you’re considering bpc 157 tb 500 capsules vs injection, you’ve probably run into the same problem I did: the labels and claims don’t tell you what actually matters—dose logistics, consistency, and whether a capsule routine is realistic for your situation. In my hands-on work with protocols (and the questions people bring to us after they’ve already started), the biggest misses aren’t “science gaps.” They’re execution gaps: timing, route selection, documentation, and knowing what tradeoffs you’re accepting.
This guide is a complete comparison of BPC-157 vs TB-500 for 2026, focused on practical decision-making. I’ll cover how the two are commonly used, what the route differences mean for outcomes, and how to choose between capsule and injection approaches without falling into hype.
BPC-157 vs TB-500: What people are trying to achieve
Before comparing routes, I like to anchor the conversation on intent. In real-world use, BPC-157 and TB-500 are typically pursued for tissue repair and recovery. People usually frame goals like:
- Faster recovery after soft-tissue strain
- Support for tendon/ligament irritation
- Managing inflammation-related discomfort
- Helping with “stalled” healing (the situation where symptoms linger)
What matters for route selection is how faithfully you can run a consistent plan. In my experience, the best protocol on paper can underperform if dosing timing slips, storage is mishandled, or tracking is missing.
Where BPC-157 typically fits
BPC-157 is commonly discussed as a peptide associated with local tissue support. Most people encounter it through practical “stacking” discussions—how it’s used alongside other recovery compounds and how it’s split across days.
Where TB-500 typically fits
TB-500 is often discussed in the context of longer-term repair pathways and recovery planning. People tend to focus on structured cycles and route-based scheduling.
Key difference: capsules vs injection (route reality, not marketing)
When people search “bpc 157 tb 500 capsules vs injection,” they usually want one decisive answer: which route is better. In practice, I treat “better” as “better for your constraints.” The route affects consistency, handling burden, and the risk of errors during administration.
Capsules: the main practical advantage
Capsules are usually preferred for:
- Ease of adherence: fewer steps, fewer failure points
- Simplicity: no mixing, fewer storage/handling steps during use
- Convenience: easier to travel with and keep routine stable
In my hands-on observations, capsule routines tend to succeed or fail based on one variable: whether the user can stay consistent. If you can’t reliably manage injection logistics (time, supplies, sterility concerns, needle fear), capsules may reduce execution error.
Injection: the main operational tradeoff
Injections are typically chosen for:
- Protocol control: you’re administering a defined delivery method
- Precision workflow: timing and dosing steps are explicit in many plans
- Route-specific planning: some users are trying to match their routine to a particular administration approach
The tradeoff is burden. I’ve seen people get derailed by practical issues: improper storage, missed doses due to day-to-day access problems, or inconsistent timing. These aren’t “small” problems—protocol interruptions can be the difference between a smooth cycle and a confusing, non-interpretable experience.
Side-by-side comparison: BPC-157 vs TB-500 across capsule vs injection considerations
Below is how I’d compare them from an execution and planning perspective (not a promise of outcomes). Use this as a decision worksheet.
| Category | BPC-157 (capsules vs injection) | TB-500 (capsules vs injection) |
|---|---|---|
| Primary user goal | Tissue support and recovery focus | Repair/recovery planning focus |
| Best fit if you want simplicity | Capsules often win for adherence | Capsules can reduce administration friction |
| Best fit if you prioritize strict protocol steps | Injection route may align with structured routines | Injection route often chosen for cycle precision |
| Execution risk (common mistakes) | Consistency lapses (missed timing, poor tracking) | Handling and administration errors; missed injection days |
| How to evaluate results | Track symptom change and function over time, not “day feelings” | Track recovery milestones and setbacks; keep notes on route adherence |
| What to decide first | Can you run the routine consistently? | Can you manage administration reliably for the full cycle? |
My hands-on lesson learned: route selection is usually a logistics decision
In one of the most common patterns I’ve seen, people choose based on online comparisons rather than their reality. For example, a client could manage capsule dosing daily but kept missing injection steps on workdays. The result wasn’t “capsules were better.” It was that adherence was higher with the option that fit the client’s schedule.
If your routine requires peak reliability, you need to audit your week: can you administer on time, store items properly, and document what you did?
Choosing between BPC-157 and TB-500: a practical decision framework
Instead of asking “which is stronger,” I suggest asking the questions that actually influence outcomes: compatibility, consistency, and interpretability.
Step 1: Define your recovery problem in measurable terms
Use functional measures whenever possible. Examples:
- How far you can move without flare-ups
- Pain scores at the same time of day
- Performance milestones (e.g., walking duration, gym movement tolerance)
Step 2: Choose the route you can execute without breaking your plan
For bpc 157 tb 500 capsules vs injection, the route should match your constraints:
- If you’re likely to miss steps, capsules may reduce execution error.
- If you’re disciplined about preparation, timing, and administration, injections may fit a structured protocol approach.
- If you’re traveling or have limited access to supplies, think hard about how “injection-ready” your life truly is.
Step 3: Track both symptoms and adherence
In my workflow, the most valuable notes aren’t just “I felt better.” They’re “I took it at X time on Y date and didn’t miss any scheduled doses.” If you can’t keep adherence notes, it becomes impossible to learn from the experiment.
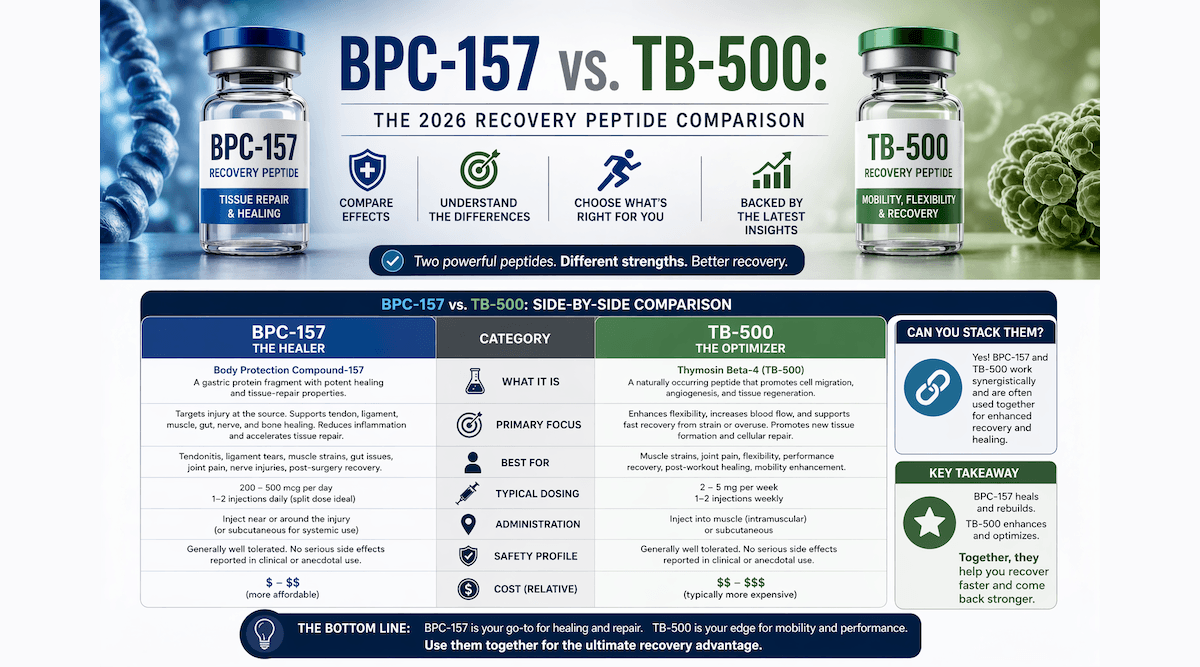
Product-image context: visual overview
Many readers land on comparison pages looking for a quick visual anchor. Here’s the product image you provided:
Capsules vs injection: pros and cons you should weigh honestly
Capsules—pros
- Lower day-to-day friction
- Fewer steps, fewer administration variables
- Easier to keep a stable routine while working or traveling
Capsules—cons
- Less “hands-on” control over administration steps
- Protocol execution can still fail if users don’t track timing and effects
- Different formulations may vary; you must understand what you’re actually taking
Injection—pros
- Structured protocol scheduling is often clearer
- Route-specific planning may be easier to implement consistently
- Precise workflow when you’re already comfortable with administration steps
Injection—cons
- More failure points (preparation, timing, storage, technique)
- Higher friction can reduce adherence over time
- Requires attention to safety practices and correct handling procedures
Common mistakes people make with BPC-157 and TB-500 protocols
- Changing too many variables at once: if you switch route and timing simultaneously, you can’t tell what affected results.
- Not documenting adherence: missed doses make your recovery timeline hard to interpret.
- Expecting immediate, day-to-day effects: recovery often changes gradually; track trends.
- Ignoring the training/sleep component: in my experience, dosing can’t “outperform” poor recovery habits.
- Relying on capsule vs injection comparisons without matching their constraints: the better option is the one you can run consistently.
FAQ
Is BPC-157 vs TB-500 better as capsules or injection?
For most people, the better route is the one they can execute consistently and safely. If your schedule and handling realistically support a structured injection routine, injection may fit. If you’re more likely to miss steps, capsules often win on adherence.
What should I track to compare outcomes fairly?
Track symptom intensity at consistent times, functional milestones (what you can do), and—most importantly—adherence (dose dates/times and any missed days). This lets you distinguish real change from noise.
Can I switch routes mid-plan?
You can, but it reduces interpretability. If you switch from capsules to injection (or vice versa), document the date of the change and expect your “before vs after” comparison to be less clean.
Conclusion: pick the route that your real life supports
BPC-157 and TB-500 are often discussed as options for recovery and tissue repair, but the capsule vs injection decision is usually won or lost on logistics. In my experience, the most actionable edge comes from choosing the route you can run consistently, defining measurable recovery markers, and tracking adherence so you can learn from what you do.
Next step: set up a simple tracking sheet today—one line per day for (1) route used, (2) dose timing, (3) pain/function measure—and run your chosen plan consistently long enough to see a trend.
Discussion