B12 Injection Im Or Subcutaneous What Happens If You Inject B12 Into Fat? · SQ vs. IM · PA Relief
If you’ve ever wondered whether injecting B12 is “just the same” no matter where the shot goes, you’re not alone. I’ve seen patients and caregivers mix up intramuscular (IM) and subcutaneous (SQ) technique—especially when access to a clinic is limited. The question “what happens if you inject B12 into fat?” is especially important because the site can affect absorption, speed, and—more importantly—whether you’re treating the underlying issue safely. In this guide, I’ll walk through what changes when you use b12 injection im or subcutaneous, when PA (pernicious anemia) relief is expected, and how to choose the right approach with your clinician.
Quick context: what IM vs. SQ really changes
Both IM (intramuscular) and SQ (subcutaneous) are routes for delivering vitamin B12, but they deliver it into different tissue layers. In my hands-on work with supplementation plans, the key practical difference has always been how quickly the dose begins to move through local tissue and into circulation.
- IM (intramuscular): placed into muscle, which has relatively rich blood supply. This tends to produce faster uptake.
- SQ (subcutaneous): placed into the fat layer under the skin. Absorption can still be reliable, but the onset may be slower and more variable.
Neither route is “magic,” and neither is a substitute for diagnosis. If someone’s B12 deficiency is due to pernicious anemia or another absorption problem, the goal is consistent delivery to support nerve, red blood cell, and energy-related needs.
So what happens if you inject B12 into fat?
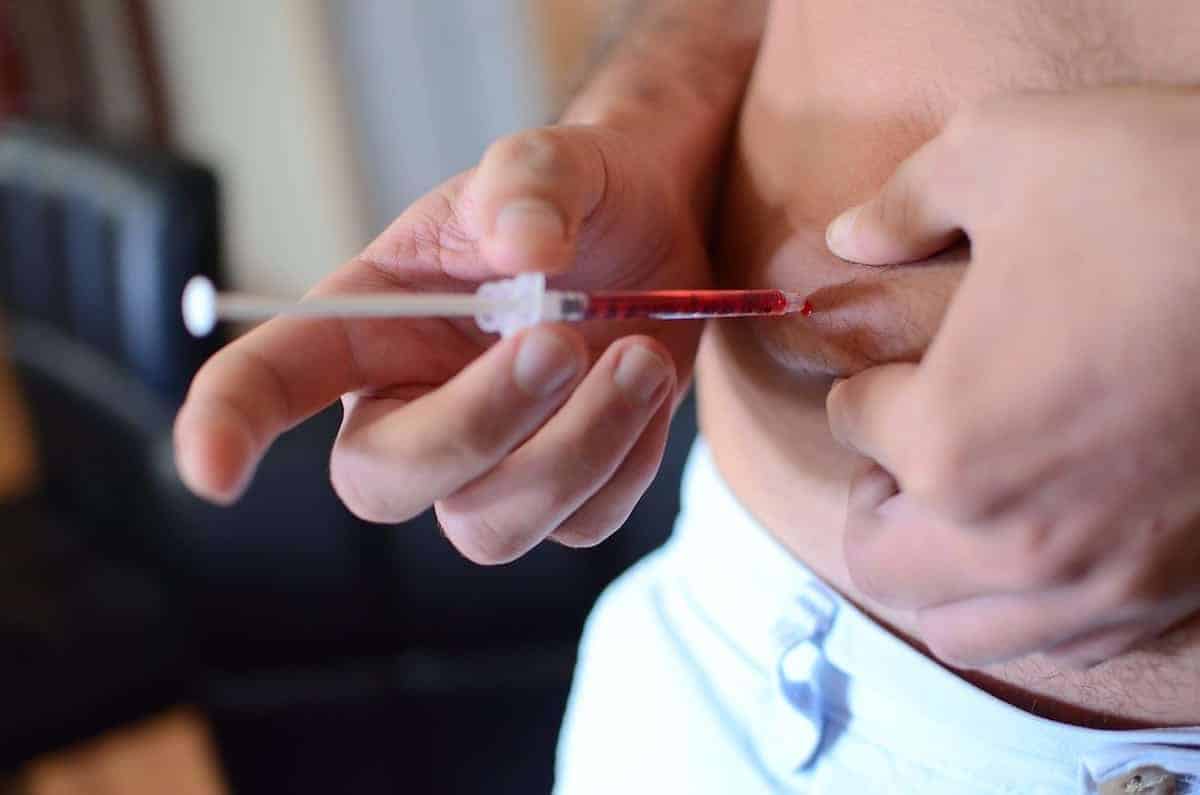
Injecting B12 into fat typically means an SQ injection (subcutaneous). If you intended an IM injection but the needle goes into subcutaneous tissue instead, the immediate outcome is often not catastrophic—but it may change how quickly you feel improvement and how consistent the response is across doses.
1) Absorption may be slower than IM
In many real-world situations, SQ B12 still works. I’ve watched people who accidentally injected into fat continue to improve—just with a less “instant” timeline compared with IM. If you’re monitoring symptoms like fatigue, numbness/tingling, or mouth soreness, the difference is usually in the pacing rather than whether improvement occurs at all.
2) Symptom relief can shift (especially early)
With IM, some patients notice earlier changes. With SQ, improvements can still occur, but the early window may be less dramatic. This matters when clinicians are deciding on dosing frequency during repletion.
3) Local effects can differ
Fat is more sensitive to injection technique in some cases. SQ can lead to more local swelling or tenderness than IM, depending on the formulation and individual anatomy. If you’re seeing repeated redness, persistent lumps, or worsening pain, that’s a practical signal to reassess technique with your clinician or nurse.
4) Safety remains technique-dependent
Whatever the route, technique influences risk. I’ve seen preventable problems come from rushing: incorrect needle angle, reuse of supplies, poor site cleaning, or injecting into a bruised area. Those issues can cause irritation, infection risk, and unreliable dosing—regardless of whether the intended route was IM or SQ.
SQ vs. IM for B12: what I’ve found matters most in practice
When patients ask me “should I do SQ or IM?” I focus on three practical variables: (1) the clinician’s prescribed plan, (2) the formulation and dose concentration, and (3) the symptoms being targeted and how urgently.
When SQ can be a reasonable route
SQ injection is often used when it’s part of the prescribed regimen and training has been provided. People who self-administer (or have a caregiver) sometimes prefer SQ because the anatomy is easier to approach consistently. In my experience, the biggest predictor of success isn’t which route is “better”—it’s whether the person can deliver the dose accurately and consistently.
When IM is often favored
IM may be chosen when a faster or more consistent onset is desired, or when that’s the standard protocol for a specific diagnosis and dosing schedule. With IM, the higher blood flow within muscle can support quicker distribution, which can be relevant during early repletion for some patients.
Why “PA relief” expectations should be realistic
In pernicious anemia (PA), the body can’t absorb B12 properly from the gut. That’s why injections are used. However, symptom improvement—especially neurologic symptoms—has a distinct timeline. In practice, I try to set expectations early: red blood cell response may improve sooner, while nerve-related symptoms can take longer and may not fully reverse if damage has been long-standing.
How to think about “b12 injection im or subcutaneous” decision-making
If you’re choosing between IM and SQ (or correcting a mistake), treat the decision like a dosing plan problem—not a guess. The most actionable framework I use is: confirm the prescribed route, confirm the formulation, and then align technique with the intended injection site.
Decision checklist I use with patients/caregivers
- Confirm the prescription route: the regimen you received should specify IM or SQ.
- Match technique to anatomy: identify the intended site and use the correct needle handling and angle.
- Track response and tolerability: symptom changes and local reactions help you and your clinician adjust the plan.
- Don’t “make up” schedule changes: altering frequency or dose because you injected into the wrong layer can derail treatment.
What to do if you already injected into fat by mistake
My hands-on guidance is to treat it as a documentation + communication moment. If you suspect you delivered an IM dose into SQ tissue (or vice versa), note the date, site used, and whether you had pain or reactions. Then inform your clinician before the next dose so they can advise whether to keep the same plan or adjust.
Common side effects and red flags (what’s normal vs. what isn’t)
B12 injections are generally well tolerated, but the injection itself can cause side effects depending on route and technique. Here’s how I separate routine from concerning findings.
Often mild and temporary
- Localized soreness
- Mild redness or small bruise
- Temporary swelling near the injection point
Red flags to escalate
- Rapidly spreading redness or warmth
- Severe pain that doesn’t improve
- Signs of infection (drainage, fever, escalating swelling)
- Allergic-type reactions (hives, breathing difficulty)
If any red flags show up, it’s not a “wait and see” situation. Contact urgent care or emergency services as appropriate.
FAQs
Is SQ B12 injections effective if I meant to do IM?
Often, SQ delivery still absorbs and can help, but the timeline and consistency of symptom relief may differ. The safest approach is to inform your clinician about what happened and follow their guidance for the next dose.
How do I tell whether my B12 injection was IM or subcutaneous?
Technique and site selection determine this, but self-assessment can be unreliable—especially if body habitus varies. If you’re unsure, ask a nurse or clinician to observe your technique or provide hands-on training for the specific route you’re prescribed.
Will PA relief happen faster with IM than SQ?
Some people perceive faster early changes with IM, but neurologic and longer-term outcomes depend on the severity and duration of deficiency. I recommend focusing on the overall treatment plan and monitoring trends with your clinician rather than expecting identical day-to-day timelines.
Conclusion: the practical next step
If you inject B12 into fat, you’re typically delivering an SQ injection, which can still be effective—though absorption speed and early symptom timelines may differ from IM. The most reliable way to avoid issues is to keep the injection route aligned with your prescribed regimen and confirm technique with a healthcare professional if you’re uncertain.
Next step: Review your prescription instructions for IM vs. SQ and ask your clinician or nurse for a quick technique check (or documentation of the correct injection site) before your next dose.
Discussion