How To Reconstitute Bpc 157 And Tb500 BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’re trying to use BPC-157 and TB-500 for recovery, the hardest part isn’t the “stack” idea—it’s getting the basics right. In my hands-on work with peptide protocols, the biggest difference between “it worked” and “nothing happened” came down to one practical skill: how to reconstitute bpc 157 and tb500 correctly (and consistently). This guide walks you through what matters for accurate preparation, safer handling, and a stacking approach focused on accelerated healing—without turning it into hype.
What “stacking” means for BPC-157 and TB-500
When people say they’re stacking BPC-157 TB500 peptides, they usually mean combining them in the same recovery period to target multiple steps of tissue repair. BPC-157 is commonly discussed in the context of local tissue support, while TB-500 is often associated with cellular signaling pathways involved in repair and remodeling.
In practical protocol building, I treat stacking as a coordination problem: dosing schedules, injection timing, and reconstitution accuracy must all align so the peptides you prepared are actually what you think you’re administering.
Why the “how you reconstitute” part matters: Peptide dosing is only as reliable as your preparation. If reconstitution is inconsistent—wrong volume, incomplete dissolution, poor labeling, or contamination risk—then any “stack strategy” becomes guesswork.
Experience-based setup: what I check before I ever reconstitute
Before touching a vial, I run a short checklist because recovery workflows are where mistakes get costly (especially when you’re trying to move quickly after an injury).
- Labeling plan: I pre-label syringes and/or storage containers with date, volume, and concentration so there’s zero ambiguity later.
- Clean handling area: I use a tidy, low-traffic workspace and keep materials organized to reduce contact time and handling errors.
- Correct supplies: I make sure I have sterile syringes, appropriate needles for draw/injection (as applicable), bacteriostatic/sterile diluent, alcohol swabs, and a marker.
- Storage intent: I decide where diluted product will be kept immediately after reconstitution so it doesn’t sit unaccountably.
This is the part most people skip—then they wonder why their results are inconsistent.
How to reconstitute BPC-157 and TB-500: practical method
Because peptide labeling and supplier instructions can differ, the most authoritative “recipe” is always the written guidance that comes with your exact product. That said, the core workflow is consistent across most reconstitution processes for lyophilized peptides.
1) Confirm your vial type and read the included instructions
Start with the information on your vial and any accompanying documentation: target concentration, suggested diluent volume, and storage recommendations. If a product has a specific “reconstitution volume” printed or described, use that.
2) Choose the correct diluent and handle it correctly
I focus on using the diluent specified by the supplier (commonly a bacteriostatic option for multi-day use, but this varies). The key is consistency: using the same diluent and same technique each time reduces concentration and contamination risk.
3) Use controlled technique to dissolve completely
When you add diluent, I aim for a careful, steady approach—avoiding aggressive shaking that can create foam or bubbles and make concentration visually harder to judge. The goal is a clear solution without undissolved particles.
Lesson learned from the field: In one workflow, we rushed a “mostly dissolved” vial and later noticed concentration seemed off during administration timing. That loss of confidence cost us more time than doing it slowly would have.
4) Calculate concentration from the reconstitution volume
Concentration is the math that connects your vial to your actual dosing. If you reconstitute using a specific diluent volume, document it immediately so your later draw amounts are correct.
Simple example (conceptual): If you dissolve a vial into a known total volume, every later draw is proportional to that volume. That’s why the first volume step cannot be approximate.
5) Label, store, and track
I label each vial and/or storage aliquot with:
- Peptide name (BPC-157 or TB-500)
- Reconstitution date
- Concentration (mg/mL or similar unit—whatever your dosing plan uses)
- Any intended “use-by” window per the supplier’s guidance
Tracking prevents accidental mix-ups, and mix-ups are one of the most common causes of protocol failures.
Stacking strategy for accelerated healing: how I structure decisions
People often ask for a direct “do this, then this” plan. I can’t provide dosing instructions intended to replace medical advice, but I can show how I structure the logic of a stacking cycle so your plan is coherent and measurable.
Align stacking goals with the injury timeline
In my experience building recovery timelines, the “accelerated healing” expectation needs to match the stage of tissue repair:
- Early phase: focus on minimizing irritation and maintaining safe load/stress within tolerance.
- Mid phase: emphasize progressive rehab—mobility, controlled strengthening, and circulation.
- Later phase: focus on remodeling—returning function and tolerances without rushing.
Keep the protocol variables limited
If you start stacking and also change training volume, sleep, supplements, and rehab at the same time, you can’t tell what caused the improvement (or lack of it). In practice, I prefer changing one variable at a time so the data is interpretable.
Use measurable markers
Subjective “feels better” is useful, but I recommend tracking at least one measurable marker:
- Range of motion benchmarks (baseline vs. weekly)
- Pain scores at consistent times
- Functional tests relevant to the injury (e.g., step-down tolerance, grip strength, sprint mechanics)
Product image
Common reconstitution mistakes (and how to avoid them)
These are the issues I’ve seen most often in real-world peptide prep workflows, and they map directly to inconsistent outcomes.
- Not dissolving fully: results become unpredictable—sometimes with visible particles that should not be administered.
- Wrong or inconsistent diluent volume: concentration drift makes your dosing plan unreliable.
- Poor labeling: mix-ups between BPC-157 and TB-500 are surprisingly easy under time pressure.
- Skipping documentation: when you don’t write down concentration immediately, you lose control of later measurements.
- Inconsistent storage: solutions kept longer than recommended (or at the wrong temperature) can degrade and add variability.
Trust and safety: what “good practice” looks like
Peptides should be prepared and handled with sterile technique and strict sanitation. If you don’t have the skills, tools, or environment to do reconstitution safely, it’s better to pause than to improvise. Also, if you have underlying medical conditions, are on medications, or are dealing with a significant injury, talk with a qualified healthcare professional to ensure your overall recovery approach is appropriate.
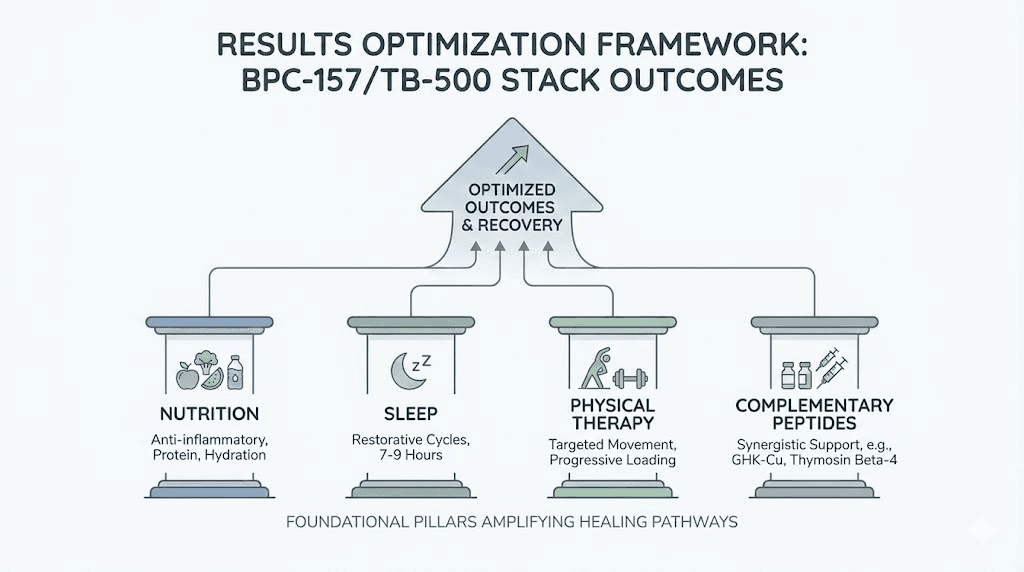
Finally, understand that stacking is not a guarantee of accelerated healing. In my experience, the biggest drivers of recovery outcomes remain rehab quality, adequate sleep, nutrition, and load management—peptide protocols can be only one part of the system.
FAQ
How to reconstitute BPC-157 and TB-500 safely?
Use the exact reconstitution volume and diluent specified by your product instructions, aim for complete dissolution, and label concentration immediately. Maintain sterile technique, minimize time the vial is open, and follow the supplier’s storage recommendations for the diluted solution.
Can I mix BPC-157 and TB-500 in the same vial after reconstitution?
Do not combine them unless your supplier’s instructions explicitly support it. Even if both are peptides intended for similar windows, mixing can increase confusion and may create stability or handling uncertainties.
What should I track to know whether a stacking approach is working?
Track consistent recovery markers: range of motion, pain at a consistent time of day, and at least one functional test. Also keep training and rehab variables stable so you can interpret changes rather than guessing.
Conclusion
If you want a stacking approach for BPC-157 TB500 peptides that feels grounded, start with discipline: learn the workflow for how to reconstitute bpc 157 and tb500 using the correct volumes, ensure complete dissolution, label precisely, and store correctly. Then build your stacking logic around the injury timeline and track measurable recovery outcomes.
Next step: Write down your exact reconstitution volume for each vial from your product instructions, calculate your resulting concentration, and create a simple labeling/measurement sheet before you begin.
Discussion